Peptides: A Comprehensive Scientific Guide for Patients

Peptides represent an important advance in modern medicine. Some peptide-based drugs have changed clinical care in meaningful ways, including treatments used for diabetes, weight management, osteoporosis, endocrine disease, and other serious conditions. These therapies can have highly specific biologic effects, which is exactly why they can be so useful when they are properly studied, properly manufactured, and used for the right indication. Not all peptides are bad. Some are highly effective and genuinely important medicines.
The problem is that the peptide world promoted on social media and online forums is very different from the peptide world supported by rigorous clinical science. Many of the peptides that are hyped online are still very early in development, have little or no meaningful human data, or have already been tested in humans and shown to be ineffective, unsafe, or simply not ready for routine clinical use. Peptides are not harmless just because they are made of amino acids. They have real biologic activity, which means they can also cause real harm. In many cases, for the goals people are chasing with unapproved peptides, there are already approved and better understood therapies that have much clearer safety profiles and much stronger clinical evidence.
Our goal in putting together this guide is to provide patients and consumers with scientific information to help them navigate the peptide landscape. We recommend individuals interested in peptides to have a discussion with a healthcare provider who has training and experience in peptides and their use in medicine.
For a more detailed discussion on peptides, you can read our article on peptides published in the scientific journal Sports Medicine here.
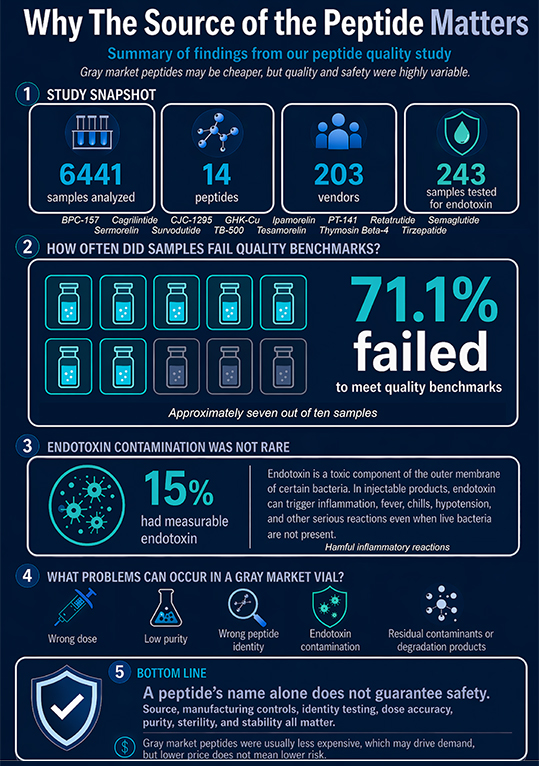
To read more on safety and sterility testing of peptides, in which we identify that 41.6% to 71.1% of gray market research grade peptides in a commercial testing dataset would not pass a few of the many basic safety standards for use in humans, click here.
What Are Peptides?
Peptides are short chains of amino acids. They sit in a middle ground between small molecule drugs and larger protein-based therapies. In the body, many peptides act as signaling molecules that help regulate metabolism, tissue repair, hormone release, inflammation, mitochondrial function, and many other biologic processes.
Some peptides are legitimate medicines with established manufacturing standards, human clinical trials, and regulatory approval. Others are sold through a gray market that uses terms like "research use only" or "not for human consumption" while still clearly targeting people who want weight loss, faster recovery, improved performance, muscle gain, or anti-aging effects. That difference matters. A peptide that has been studied, manufactured properly, and prescribed appropriately is very different from a peptide bought online from an unregulated seller.
FDA Approval Of Peptides

One reason to be cautious about many unapproved peptides is that FDA approval is not just a paperwork step. It usually reflects a long process designed to answer basic but critical questions. Does the drug actually work for the condition it is being marketed for? What dose is appropriate? What short term and longer term side effects show up in humans? How often do serious adverse events occur? Can the product be manufactured consistently with the right identity, purity, stability, and sterility? Only 1 in 5000 drugs that start off in lab and animal testing make it to being approved in humans.
For a new drug, development usually starts with laboratory work and preclinical testing, including animal studies, before the sponsor files an Investigational New Drug application to begin human trials. Clinical testing then typically moves through Phase 1 trials, which focus mainly on safety and dosing, Phase 2 trials, which look at early efficacy and continue safety evaluation, and Phase 3 trials, which are larger studies designed to determine whether the drug provides a real clinical benefit and to better define the risk profile. After that, the sponsor submits a New Drug Application, and FDA reviewers examine the clinical data, manufacturing information, and proposed labeling before deciding whether the benefits outweigh the known and potential risks for the intended population. FDA also continues post-market safety monitoring after approval.
That process matters because it creates a much clearer picture of how a drug behaves in real patients. Many peptides hyped online never make it through that pathway. Some reach human testing and fail because they do not work well enough or because the safety profile is not acceptable. And even when a peptide itself is promising, a vial sold through an unreliable online source is still not equivalent to an approved drug made under regulated manufacturing standards. That is why approval status, clinical trial quality, and manufacturing quality all need to be part of the conversation.
Social Media Amplifies The Placebo Effect Of Peptides

One of the most important things to understand about peptides is that the effect people feel from them is not always explained by the peptide alone. The placebo effect and the broader contextual effects of treatment can strongly influence how someone experiences pain, recovery, energy, performance, and wellness. Peptides are especially good at generating these effects because they are often presented as advanced, cutting edge, insider therapies. They are injectable, complex sounding, and promoted as something that conventional medicine is supposedly ignoring. That combination can create a powerful expectation of benefit.
Social media platforms magnify this problem. On Instagram, TikTok, YouTube, Reddit, and online forums, peptides are often discussed in a highly selective way. People talk about faster healing, better workouts, improved body composition, and dramatic recovery stories. This is similar to the hype around snake oil elixirs at the turn of the century. What is usually missing is a serious discussion of contamination, poor manufacturing, inaccurate dosing, cancer related concerns, endocrine disruption, metabolic side effects, vascular effects, organ effects, or the simple fact that many of these compounds have barely been studied in humans at all. Every drug has side effects. Every biologically active therapy has tradeoffs. Peptides are no exception, but the downside is often ignored when these compounds are hyped online.
This creates a feedback loop. Once someone starts clicking on peptide related content, algorithms tend to fill their feed with more of the same. The message becomes repetitive and persuasive. More hype leads to more expectation. More expectation can amplify the placebo and contextual effects. That can make a compound seem much more effective than the actual human evidence would support. This does not mean people are inventing their experiences. It means subjective improvement is not the same thing as good science, especially when the surrounding environment is built to intensify belief and minimize skepticism. If a peptide is not effective but is safe to use, then the placebo effect might actually be helpful in achieving desired therapeutic or wellness goals. But the placebo effect doesn't work two ways -- the placebo effect does not protect against the harm that can come from unsafe peptides.
Why The Source Of The Peptide Matters – Avoid The Grey Market
Even when a peptide itself has a legitimate medical role, the source still matters enormously. A safe and effective peptide manufactured under regulated conditions is not the same thing as a peptide purchased online from an unreliable supplier. Peptides made outside proper manufacturing systems may contain contaminants, endotoxin, heavy metals, residual solvents, microbial contamination, degradation products, the wrong concentration, or even the wrong amino acid sequence.
That last point is especially important. A peptide is not just defined by its name. It is defined by its exact amino acid sequence, its purity, its formulation, and its stability. Even a small sequence disruption can change how a peptide behaves biologically. In some cases, that could make the peptide ineffective. In other cases, it could make it unpredictable or harmful. This is why “safe peptide” and “safe vial bought online” are not the same thing.
This distinction matters because some patients assume that if a peptide has been used in medicine somewhere, any version of that peptide must also be safe. That is not how pharmaceutical quality works. Identity, purity, sterility, stability, and batch consistency are not minor details. They are central to whether a drug behaves the way clinicians and patients think it will behave.
Approved peptides can be produced by commercial manufacturers (“pharma”), or in some cases by compounding pharmacies. A compounding pharmacy can take a raw source, bulk peptide drug and prepare it for individual patient use. The United States Pharmacopeia (USP) is an organization that sets important regulatory and safety standards for drug manufacturing and production, and compounding pharmacies must follow USP guidelines when preparing compounded peptides.
There is an emerging “gray market” of peptides which are not subject to regulatory oversight. Approved peptide drugs are made under highly controlled conditions with strict purification, identity testing, batch validation, and contamination monitoring. Gray market peptides are often produced outside those systems. That means the vial may contain the wrong dose, the wrong peptide, breakdown products, residual solvents from synthesis, bacterial contamination, endotoxin contamination, heavy metals, or other impurities that would normally be detected and removed in regulated manufacturing. Even a vial labeled “99 percent pure” may still contain clinically important impurities if the manufacturing and validation process is poor.
Stability is another issue. Peptides are not all equally stable. Some can degrade with heat, light, repeated reconstitution, storage errors, or prolonged time in solution. Once a peptide breaks down, the biologic effects may become weaker, unpredictable, or potentially harmful. This is another reason why buying peptides from uncontrolled sources is risky. You are often trusting the label without any meaningful proof of identity, sterility, or stability.
Safety And Purity Testing of Peptides

When a peptide is made for the regulated US drug market, testing is usually much broader and more standardized than a simple spot check. Instead of relying on one report that looks at only a few features, regulated peptide products are typically evaluated within a larger quality system that may include identity testing, assay or potency testing, impurity testing, and, for injectable products, sterility and endotoxin testing. USP standards and reference materials are often part of that process, and FDA quality requirements also involve written specifications, lot release testing, process controls, documentation, and stability work. The goal is not just to show that the main compound is present, but to make sure the product is consistent, controlled, and as safe as possible.
That broader framework adds cost, but it also adds protection. Regulated peptide products are more expensive in part because manufacturers are paying for validated methods, specialized equipment, microbiological controls, reference standards, trained personnel, batch review, and ongoing quality oversight throughout the manufacturing process. By contrast, gray market peptides can often be sold at a lower price because they are commonly made and released with much less testing, less documentation, and less control over the full process. Lower cost may sound attractive, but part of that lower cost often comes from doing less work to look for problems before the product reaches the buyer.
Labs that commonly test gray market peptides such as Janoshik, Krause Analytical, and BTLabs can still provide useful information, but the testing they offer is usually far more narrow and limited than USP testing. Identity, amount, and peptide purity may be part of a standard peptide report, while endotoxin, sterility, heavy metals, and peptide-contamination screening are not commonly performed. Peptide contamination screening is limited to peptides on predetermined lists and is subject to considerable error. These reports can be helpful, but they are still not the same as the full release and quality framework used for regulated drug products.
Amino acid sequence is another important reason that limited testing can miss meaningful problems. Many gray market peptide reports are centered on methods such as HPLC and routine LC-MS identity testing. Those approaches can suggest that the main compound looks close to the expected peptide, but they do not always prove, residue by residue, that every amino acid in every molecule is correct. More advanced sequence confirmation often requires MS/MS peptide mapping or other higher-level structural work, and even then sequence coverage can be incomplete unless the method is specifically designed for that purpose. This matters because a single amino acid substitution, especially if present only at a low level, may change how a peptide binds, how stable it is, how it breaks down, or whether it is more likely to trigger an unwanted immune response. In other words, a product can look acceptable on a basic report while still containing a subtle sequence problem that changes how it behaves in the body.
This is why people who are careful about toxins, contaminants, and hidden ingredients in their food and everyday lives should care even more about peptide quality. A product can look reassuring on a limited lab report while still containing something important that was never tested for, never fully identified, or not measured in enough detail. Even a small amount of the wrong impurity, or a subtle sequence error, can matter, especially if the product is injected. The closer something gets to going directly into the body, the more important it becomes to know not just that the main ingredient appears to be present, but how thoroughly the product was actually tested.
List of Peptides and Their Function
The following is a list of peptides, including a brief background, how the peptide is thought to work, a summary of the in vitro (ie studies done on cells grown in a dish or in a test tube) and animal model data, results from human studies, FDA approval status, and alternatives to that peptide that might be considered for treating specific conditions.
Click on the tabs below to explore more information.
AOD-9604
Brief Background
AOD-9604 is a peptide fragment derived from human growth hormone. It was originally developed to capture the fat loss effects of growth hormone without the broader anabolic and insulin related effects of full growth hormone exposure. For that reason, it attracted interest as a possible obesity treatment and later began circulating in wellness and peptide communities as a weight loss and body composition drug. More recently, some people have tried to extend its use into joint and cartilage related conditions, but that shift has occurred with very little human clinical support.
AOD-9604 is a good example of a peptide that sounds more exciting online than it looks when you review the actual development history. Unlike many gray market peptides, it was at least studied seriously enough to reach human clinical trials. But that is also what makes it informative. Once it was tested in people, the results did not support the kind of meaningful weight loss benefit that would justify broad clinical use. Basically, AOD-9604 appears to be safe, but hundreds of millions of dollars of clinical research demonstrated it is ineffective for weight loss. Despite the overwhelming evidence showing this lack of effect on body weight, it is still heavily marketed by influencers on social media.
How The Peptide Works
AOD-9604 is thought to work primarily through beta adrenergic signaling and lipolytic pathways. The original idea was that this fragment of growth hormone could promote fat breakdown without strongly activating the full growth hormone receptor or significantly increasing IGF-1. That made it appealing as a possible "cleaner" metabolic peptide, at least in theory. That said, even a more limited mechanism does not make it automatically useful or harmless. If a peptide is pushing adrenergic or metabolic signaling, there is still potential for unintended physiologic effects. One of the concerns is that prolonged activation of these pathways could theoretically contribute to dysautonomia related symptoms, especially if used chronically or outside controlled settings.
Summary Of In Vitro And Animal Model Studies
Preclinical work on AOD-9604 suggested it could reduce fat mass in animal models of obesity. Those findings helped justify early interest in developing it for weight loss. There has also been some preclinical interest in cartilage repair, including animal work in osteoarthritis models, which likely helped fuel later online claims that it might help joints or cartilage healing.
But this is another example of why animal data should be interpreted carefully. A peptide can look promising in rodents and still fail to become a clinically useful drug. That is exactly what appears to have happened here. The preclinical story was good enough to justify more study in clinical trials, but when studies were conducted in humans, it was clear that AOD-9604 was ineffective as a therapy.
Summary Of Human Studies
AOD-9604 was evaluated in multiple randomized, double blind, placebo controlled human trials for obesity, involving hundreds of patients. That is already more human data than exists for many of the peptides discussed online. The short-term safety profile appeared reasonably favorable in those studies, and there were no major signals suggesting growth hormone like increases in IGF-1 or worsening insulin sensitivity.
The problem is that the peptide did not show a convincing, dose dependent, clinically meaningful effect on weight loss. In other words, it appears to have been studied enough to show that while it may not be dramatically dangerous in the short term, it also was not effective enough to justify approval as a weight loss drug. That is an important distinction, because many people online talk about AOD-9604 as if it is a proven fat loss agent when the human trial results do not support that view.
FDA Approval Status
AOD-9604 is not FDA approved. FDA materials from the December 2024 Pharmacy Compounding Advisory Committee meeting state that FDA proposed AOD-9604 free base and AOD-9604 acetate not be included on the 503A bulks list, and FDA briefing materials note characterization, impurity, immunogenicity, and degradation concerns for these substances.
One practical issue with AOD-9604 is that peptide stability and formulation matter. FDA briefing materials specifically note degradation and aggregation concerns, along with limited characterization data and the absence of a USP drug substance monograph. That means even apart from the question of efficacy, there are also quality and formulation concerns when this peptide appears in compounding or gray market channels.
Alternatives
If the goal is meaningful weight loss, AOD-9604 is not a strong option. GLP-1 receptor agonists are much better supported and dramatically more effective. Phentermine may also be a reasonable option in selected patients, depending on the clinical situation. If the goal is improving joint pain or arthritis related symptoms, the better strategy is to treat the actual condition using evidence-based approaches rather than trying to repurpose an ineffective obesity peptide.
If the interest in AOD-9604 is really about body composition more broadly, the foundation should still be nutrition, resistance training, sleep, and evidence based medical treatment when indicated. The main lesson from AOD-9604 is that a peptide can sound elegant mechanistically and still fail where it matters most, which is helping real patients achieve meaningful outcomes.
BPC-157
Brief Background
BPC-157, short for "Body Protection Compound-157," is a 15 amino acid peptide that has become one of the most widely discussed gray market peptides in health and wellness. It is a fragment of a patented, incompletely characterized gastric juice protein. BPC-157 is promoted online for tendon healing, ligament recovery, muscle injury, joint pain, gut health, and general tissue repair. Its reputation has been built much more by animal studies, repeated online testimonials, podcast culture, and social media hype than by rigorous human clinical science. It is supposedly found in human gastric juice and thought to protect the stomach from acidic conditions, but no human proteomic study has independently identified any peptides similar to BPC-157, and the sequence does not correspond to any known gene in the human genome.
One reason BPC-157 has become so controversial is that the amount of enthusiasm around it is far out of proportion to the quality of the evidence. BPC-157 was first reported in 1993, and while there are over 150 published primary research papers on BPC-157, almost all of the animal studies come from a single lab at the University of Zagreb in Croatia. There is no moderate or high quality human data, and frequently repeated claims about clinical use are not backed by the kind of transparent, peer reviewed human outcome studies clinicians would normally want to see before taking a treatment seriously. That does not automatically prove the peptide is ineffective, but it does mean consumers should be much more cautious than the online conversation usually suggests, especially since most of the data come from a few labs, despite the peptide being known for years.
How The Peptide Is Thought To Work
BPC-157 is thought to work through several biologic pathways, but the most commonly discussed mechanisms involve activation of the VEGF pathway. VEGF signaling can promote new blood vessel formation, vascular regulation, nitric oxide related effects, and inflammatory modulation. In practical terms, BPC-157 is often described as a peptide that may promote blood vessel formation, improve tissue perfusion, and support tissue remodeling after injury. Those proposed actions help explain why it is so heavily marketed for tendons, ligaments, muscle, and other connective tissues.
The problem is that a plausible mechanism is not the same thing as proven clinical benefit. Some of the same biologic activities that sound attractive in marketing can also raise concern. VEGF activation is not automatically beneficial in every tissue or every disease state. Indeed, VEGF signaling plays a central role in cancer metastasis. No other drug that has activated VEGF safely has made it to market, most have been tremendous failures. And one of the biggest blockbuster cancer drugs in the past few decades is Avastin, which blocks VEGF. So activating VEGF can promote cancer growth and metastasis, while blocking it can limit these processes. Pathways involved in blood vessel growth are also not necessarily favorable in chronic tendinopathy, where it is associated with worse tissue quality or symptoms. In other words, the mechanism that gets marketed as "healing" may also carry biologic tradeoffs that are almost never discussed online.
Summary Of In Vitro And Animal Model Studies
Preclinical data are the main reason BPC-157 became popular. In vitro and animal model studies suggest it may improve healing responses in tendons, ligaments, muscle, gastrointestinal tissue, liver, gut, heart, spinal cord, nerve, glaucoma, and many others. BPC-157 seemingly improves healing for virtually every tissue it has been studied in. Rodent studies have described increased blood vessel growth, reduced inflammatory signaling, and better recovery in a variety of injury models. These findings help explain why so many people became excited about the peptide.
At the same time, this is exactly where many experimental drugs look their best. Animal data are useful for generating hypotheses, but they are not enough to justify routine human use. Many compounds that appear promising before or early in human testing never become successful therapies once they are studied carefully in people. That gap between preclinical promise and clinical reality is one of the most important reasons to be cautious with BPC-157. Certainly, something with such profound positive effects on the healing of every tissue in the body, and was discovered over 20 years ago should have easily made it through clinical trials by now? If we compare BPC-157 to the GLP-1 peptides like semaglutide and tirzepatide, they were discovered several years after BPC-157, with now a few thousand studies in animal or in vitro models by hundreds of different independent labs around the world.
Summary Of Human Studies
Human evidence for BPC-157 remains extremely limited. There is one published study in knee osteoarthritis, where BPC-157 was randomly injected into knee joints, and patients were called up to a year later to ask them how their knee felt. This study would not make it into the vast majority of recognized scientific journals. There was another study where BPC-157 was injected into the bladder of patients with interstitial cystitis, and the authors noted that everyone in the study felt better after the treatment. But often times interstitial cystitis resolves on its own. The study did not use standardized outcome instruments in urology and used an experimental design that makes it impossible to determine if BPC-157 actually had an impact on bladder healing.
There were two registered clinical trials that were conducted of BPC-157. Both trials were abandoned with no results posted. For one of the trials, data was submitted before it was later withdrawn. When this happens, it usually doesn't occur because something positive happened in the trial.
That matters because BPC-157 is often discussed online as if its benefits are already settled science. They are not. At this point, there is still too little reliable human evidence showing how it works in people, whether it is effective for the conditions it is marketed for, or what the true short term and long-term safety profile looks like in real world use.
FDA Approval Status
BPC-157 is not FDA approved. There are also regulatory concerns around its use in compounding, including limited safety information for proposed routes of administration, uncertainty related to peptide impurities and active ingredient characterization, and concern that there is not enough reassuring information to conclude that it can be used safely in humans. Despite that, it remains widely available through gray market and adjacent sales channels, which creates a misleading sense of legitimacy for consumers.
Alternatives
The right alternative depends on the actual goal. If someone is looking for tendon, ligament, or muscle recovery, evidence based rehabilitation, progressive loading, and condition specific physical medicine approaches are much better supported. Depending on the condition, other options may include shockwave therapy, platelet rich plasma, platelet poor plasma, or cell therapies like bone marrow aspirate, microfat, or stromal vascular fraction treatments. These therapies all have solid, evidence-based studies to back their use.
CJC-1295
Brief Background
CJC-1295 is a synthetic growth hormone releasing hormone analog designed to stimulate the release of growth hormone from the pituitary gland. It became popular in gray market and performance medicine circles because it is marketed as a way to increase growth hormone, reduce fat, improve recovery, and support muscle gain without directly injecting growth hormone itself. It is often discussed alongside ipamorelin, with the idea that combining the two will create a more powerful or more "physiologic" increase in growth hormone signaling.
One reason CJC-1295 became so popular online is that it sounds scientifically sophisticated. It acts upstream of growth hormone, it has a long half-life, and it fits neatly into the broader anti-aging and body composition narrative that dominates peptide culture. But when you look more carefully, the story becomes much less reassuring. This is not a benign wellness tool. It is a peptide with real endocrine effects, that was investigated in clinical trials and abandoned due to safety concerns.
How The Peptide Is Thought To Work
CJC-1295 works by binding to growth hormone releasing hormone receptors in the pituitary gland, which stimulates growth hormone secretion and increases IGF-1 levels downstream. Unlike the body's natural pulses of growth hormone releasing hormone, CJC-1295 was designed to have a prolonged duration of action. That means it can drive a more sustained increase in growth hormone signaling than the normal physiologic pattern.
That prolonged effect is one of the reasons people use it, but it is also one of the main reasons to be cautious. Growth hormone physiology is normally pulsatile and tightly regulated. If you push the system too hard or too continuously, you can move away from normal signaling and into a more pharmacologic state that may promote unwanted effects. Chronic activation of the growth hormone and IGF-1 axis can contribute to water retention, insulin resistance, altered glucose handling, and possibly more serious downstream consequences if used over longer periods. Putting growth hormone "on blast" may sound good in social media posts, but the reality is, there is a medical condition called acromegaly where growth hormone levels become really high. These patients suffer from joint pain, enlarged hearts, higher risk of heart disease and strokes, and early mortality.
Summary Of In Vitro And Animal Model Studies
The rationale for CJC-1295 is based much more on endocrine manipulation than on direct tissue-specific healing data. Its appeal is not that it has dramatic preclinical studies showing direct repair of tendon, ligament, or muscle. Instead, it is built on the assumption that raising growth hormone and IGF-1 should help improve body composition, recovery, and possibly tissue healing.
That assumption is biologically plausible, but it is often overstated. There is a difference between a hormone pathway being involved in tissue adaptation and a synthetic peptide safely improving outcomes in real patients. CJC-1295 is a good example of a compound where the mechanistic theory sounds much stronger than the actual outcome evidence.
Summary Of Human Studies
Human studies show that CJC-1295 can produce a marked and prolonged increase in growth hormone levels, with increases persisting for several days after a single injection. That confirms the drug is biologically active. But biologic activity is not the same thing as a favorable risk-benefit profile. In dose escalation work, considerable adverse events were very common, occurring in most participants who received the peptide.
There was also a phase II trial in HIV associated lipodystrophy that was halted after a patient death, although the exact role of CJC-1295 in that event remained debated. After receiving the 11th weekly dose of CJC-1295, the patient complained of chest discomfort, experienced a heart attack, and died approximately one hour later. Even if causality was not clearly established, that is not the kind of clinical history that supports treating this peptide as a casual body composition or anti-aging tool. The side effects and potential death led the company that owned the patent on CJC-1295 to abandon development, likely because there was not a clear and safe path to approving the drug. In our analysis of influencers who have promoted CJC-1295, often with links to purchase a "research grade" compound in their profile, there is no mention of the high rate of side effects and death in early clinical trials of the peptide.
It is also important to remember that while CJC-1295 clearly raises growth hormone, there is not strong human evidence showing that it safely delivers the dramatic muscle gain, fat loss, or recovery benefits often promised online. Everything we know about the biology of HGH would suggest that there would be no effect on muscle growth, and limited effects on fat loss.
FDA Approval Status
CJC-1295 is not FDA approved. It is also among the peptides that FDA has identified as presenting significant safety concerns in the compounding context. This matters because many patients assume that if a peptide is widely available through anti-aging clinics, online vendors, or compounding adjacent channels, it must have some legitimate clinical standing. That is not true. Availability is not the same thing as approval, safety, or good evidence.
Alternatives
The right alternative depends on the actual goal. If someone is looking for weight loss or fat reduction, GLP-1 receptor agonists and phentermine are much better supported and far more clinically established. If the goal is preserving or rebuilding muscle, the foundation should be progressive resistance training, adequate protein intake, sleep, and management of the condition causing muscle loss in the first place. Testosterone or anabolic agents may be able to help in some conditions.
If someone is interested in CJC-1295 because they are chasing improved recovery or better body composition, there are safer and more evidence-based approaches than prolonged manipulation of the growth hormone axis. In selected patients with true endocrine issues, there may be appropriate medical strategies to address those problems directly. But for the typical online use case, CJC-1295 is a high risk and poorly justified shortcut rather than a well-supported therapy.
Delta Sleep Inducing Peptide (DSIP)
Brief Background
Delta Sleep Inducing Peptide (DSIP) is a small neuropeptide that has been discussed for decades in relation to sleep, stress physiology, pain, endocrine regulation, and recovery. In peptide and wellness spaces, it is usually marketed for deeper sleep, better recovery, improved resilience to stress, and sometimes broader performance or hormone related effects. DSIP has an unusually long history compared with many newer gray market peptides, but that history should not be confused with strong modern clinical validation. The literature is old, relatively small, and much less definitive than the online discussion usually suggests.
Part of what makes DSIP confusing is that it has been studied enough to sound legitimate, but not enough to be treated like an established mainstream therapy. It is not in the same category as a completely evidence-free peptide, but it is also not an FDA approved sleep medication with a clear modern development program. That puts it in the familiar gray zone where a peptide can accumulate a strong reputation long before it accumulates strong clinical proof.
How The Peptide Is Thought To Work
DSIP is thought to influence sleep regulation and broader neuroendocrine physiology, but its mechanism has never been fully settled. Older research has linked it to sleep architecture, stress responses, autonomic function, pain modulation, and growth hormone related physiology. One of the challenges with DSIP is that even after years of study, investigators have continued to describe it as something of an unresolved puzzle rather than a cleanly defined therapeutic mechanism.
That uncertainty matters. A peptide can have interesting biologic effects without being a reliable or well characterized drug. In the case of DSIP, the theory is attractive because it appears connected to slow wave sleep and recovery related physiology, but the underlying biology is still not straightforward enough to support the kind of confident claims that are often made online.
Summary Of In Vitro And Animal Model Studies
Preclinical and experimental work helped create the idea that DSIP may influence slow wave sleep, stress responses, and endocrine signaling. Animal studies and mechanistic work have suggested links between DSIP related signaling and sleep associated growth hormone release, along with broader physiologic effects beyond sleep alone. These findings are the main reason DSIP developed a reputation as a recovery or sleep peptide rather than just a niche neuroscience curiosity.
At the same time, the preclinical story is not as clean as the marketing usually implies. DSIP has long been difficult to pin down biologically, and even the existence and role of endogenous DSIP like signaling have been debated. That does not mean the peptide is useless. It means the underlying science is more unsettled than people assume when they hear it described as a proven deep sleep peptide.
Summary Of Human Studies
Human studies on DSIP do exist, and some of the older sleep literature is more encouraging than what is seen with many gray market peptides. Small studies in people with insomnia reported improvements in sleep and, in some cases, daytime functioning, particularly in patients with disturbed sleep rather than in healthy sleepers. There were also early open label and double-blind studies that suggested DSIP could have sleep normalizing effects in selected insomnia populations.
But the limitations are obvious. These are older studies, generally small, and not part of a large modern clinical development program that would support widespread routine use today. Human findings have also not been uniformly simple or reassuring. In one later human study, DSIP altered bispectral index and autonomic measures in ways that did not cleanly fit the popular image of a peptide that simply deepens restorative delta sleep.
FDA Approval Status
DSIP is not FDA approved. FDA's current page on certain bulk drug substances that may present significant safety risks does not show DSIP as an approved therapeutic peptide, and there is no FDA approved DSIP drug product for sleep, recovery, or performance.
Alternatives
If the goal is insomnia or poor sleep quality, the better supported options usually include cognitive behavioral therapy for insomnia, sleep hygiene, circadian rhythm interventions, treatment of sleep apnea when present, and standard sleep medications when clinically appropriate. If the problem is daytime fatigue rather than insomnia, the more rational first step is to identify why energy is low in the first place, which may involve sleep debt, iron deficiency, endocrine issues, medications, depression, anxiety, or overtraining rather than a deficiency of an experimental peptide.
If the goal is better recovery or stress resilience, the evidence base still favors basics over peptides. Sleep regularity, carbohydrate availability around training, creatine when appropriate, management of training load, and treatment of underlying medical or psychiatric contributors are all more established than DSIP. The broader point is that DSIP is biologically interesting, but for most of the outcomes people hope to get from it, there are already safer and better characterized ways to approach the problem.
GHK-Cu
Brief Background
GHK-Cu, short for glycyl-L-histidyl-L-lysine copper, is a naturally occurring copper binding peptide that has been discussed for years in skin care and cosmetic medicine. It is often marketed for collagen support, skin rejuvenation, wound healing, hair related benefits, and more recently for joint pain and general wellness. Online discussions frequently blur together very different uses of GHK-Cu, which is a major source of confusion. Topical cosmetic use is very different from injectable or oral use, both biologically and from a safety standpoint.
This is one of the better examples of how a peptide can have a legitimate lower risk niche in one setting and become much more questionable once people start using it in ways that were never well studied. Topical GHK-Cu has a long history of cosmetic use, but that should not be used to imply that oral or injectable GHK-Cu is safe, effective, or medically established. Those are very different claims.
How The Peptide Is Thought To Work
GHK-Cu is thought to work through effects on collagen biology, wound healing pathways, inflammatory signaling, and tissue remodeling. It has also been described as having antioxidant effects and as influencing gene expression related to repair and skin quality. These proposed actions help explain why it is commonly marketed for skin, hair, and cosmetic applications.
The copper component is central to how the compound is thought to function, but that is also where some of the concern begins. Copper is an essential trace metal, but like many biologically active substances, it can be beneficial in the right context and harmful in the wrong one. Once people move away from topical exposure and into oral or injectable use, the biologic meaning of "copper peptide" changes substantially, and the possibility of toxicity or unintended tissue effects becomes much more relevant.
Summary Of In Vitro And Animal Model Studies
Preclinical work suggests GHK-Cu may support collagen synthesis, wound healing, angiogenesis, and anti-inflammatory signaling when applied topically in the skin. These findings have helped build the reputation of GHK-Cu as a regenerative or restorative peptide, especially in aesthetic medicine and anti-aging spaces. The preclinical story is one reason the peptide continues to attract interest.
At the same time, most of the enthusiasm is strongest for surface tissues such as skin, where topical exposure is the main use case. That does not automatically justify extrapolating the peptide into oral or injectable wellness applications. Many compounds look favorable in cell culture, laboratory systems, or preclinical skin related models, but that is very different from establishing safe systemic use in humans.
Summary Of Human Studies
Human use of GHK-Cu is most credible in the topical cosmetic setting. Topical formulations have been used for skin quality, texture, and appearance, and this is the context in which the peptide has the longest practical history. That does not mean it is an approved drug for those purposes, but it does mean the lower risk and more defensible use case is topical rather than systemic.
By contrast, there is little convincing human evidence supporting oral or injectable GHK-Cu for joint healing, musculoskeletal recovery, general wellness, or systemic rejuvenation. Once people start taking it by mouth or injecting it, the evidence base drops off substantially. Oral use would likely immediately degrade the GHK peptide and release free copper into the stomach. Similarly, small peptides like GHK are likely to be degraded in synovial fluid, releasing free copper into the joint. Copper causes inflammation and programmed cell death in the synovial and cartilage cells in the joint. While clinical trials have not been conducted, based on what we know about the science of copper in the joint, GHK-Cu would likely contribute to joint erosion rather than supporting healing.
FDA Approval Status
GHK-Cu is not FDA approved as a drug. In the United States, cosmetic products and cosmetic ingredients generally do not go through FDA premarket approval. That means a topical cosmetic product containing GHK-Cu is not the same thing as an FDA approved medication. It may still be marketed as a cosmetic, but that should not be confused with drug approval or proof of clinical efficacy.
Injectable GHK-Cu is much more concerning from a regulatory standpoint. FDA has specifically included GHK-Cu for injectable routes of administration on its list of bulk drug substances that may present significant safety risks in the 503A compounding context. That should make consumers and clinicians much more cautious about compounded or gray market injectable versions.
Alternatives
The right alternative depends on the reason someone is interested in GHK-Cu. If the goal is joint pain or musculoskeletal recovery, the better approach is usually to focus on the actual condition being treated and use evidence based options such as rehabilitation, progressive loading, shockwave therapy, platelet rich plasma, or selected cell based therapies depending on the indication.
Incretins/GLP-1s (Semaglutide, Tirzepatide, CagriSema, Retatrutide)
Brief Background
Incretin based drugs are among the most important peptide advances in modern medicine. These drugs grew out of gut hormone and exercise biology, and have changed the treatment landscape for obesity, type 2 diabetes, and cardiometabolic disease. These drugs are designed to activate the glucagon-like peptide 1 (GLP-1) receptor. GLP-1 is a natural hormone produced from a larger protein called proglucagon. It is released mainly by cells in the lower small intestine and colon after a meal, although exercise can also increase levels. GLP-1 helps control blood sugar, slows how quickly food leaves the stomach, reduces the release of glucagon, and helps individuals feel full. Together, these effects make it an important hormone for appetite, metabolism, and energy balance.
Semaglutide and tirzepatide are already established therapies with FDA approvals in major metabolic indications. CagriSema and retatrutide are newer agents in late-stage development that are drawing attention because they appear capable of producing even greater weight loss and broader metabolic effects. This is a completely different category from the gray market peptides discussed elsewhere in the article. These are serious drug development programs with large clinical trials, standardized manufacturing, and real regulatory scrutiny.
Semaglutide is a GLP-1 receptor agonist and is FDA approved in different branded forms for type 2 diabetes and chronic weight management. Wegovy is also FDA approved for reducing major adverse cardiovascular events in certain patients with obesity or overweight and established cardiovascular disease, and in 2025 it also gained FDA approval for metabolic dysfunction-associated steatohepatitis (MASH) in adults with moderate to advanced fibrosis. Tirzepatide is a dual GIP and GLP-1 receptor agonist that is FDA approved as Mounjaro for type 2 diabetes and as Zepbound for chronic weight management. Zepbound is also FDA approved for moderate to severe obstructive sleep apnea in adults with obesity. CagriSema is a fixed dose combination of semaglutide and cagrilintide that has been submitted to FDA for weight management and remains investigational. Retatrutide is a triple agonist targeting GLP-1, GIP, and glucagon receptors and remains investigational, although phase 3 results are now emerging.
How The Peptides Are Thought To Work
Semaglutide works by activating the GLP-1 receptor. In practical terms, this slows gastric emptying, increases satiety, reduces caloric intake, improves glucose control, and contributes to meaningful weight loss. Tirzepatide builds on this by activating both GIP and GLP-1 receptors, which appears to enhance metabolic effects beyond GLP-1 agonism alone. CagriSema combines semaglutide with cagrilintide, an amylin analog, with the goal of using two complementary satiety and metabolic pathways together. Retatrutide goes even further by combining GLP-1, GIP, and glucagon receptor agonism, which is designed to affect appetite, glycemia, and energy expenditure at the same time.
This matters because these agents are not vague "fat loss peptides." They are highly active endocrine and metabolic drugs. That is exactly why they can be so effective, but also why they can cause real side effects and require proper medical supervision. Semaglutide and tirzepatide both carry boxed warnings about thyroid C cell tumors in rodents, and both have known gastrointestinal adverse effects and other important warnings in FDA labeling. Their clinical value comes not from being risk free, but from the fact that the benefits and risks have been studied carefully in large human trials and formal regulatory review.
Summary Of In Vitro And Animal Model Studies
The preclinical story for incretins is much stronger and more coherent than what is seen with most gray market peptides. The biology of GLP-1, GIP, amylin, and glucagon signaling has been studied extensively in metabolic disease, appetite regulation, and energy balance. These pathways have direct relevance to obesity, glycemic control, cardiovascular risk, and fatty liver disease. That is one reason these drugs translated into legitimate clinical therapies rather than staying stuck in the experimental stage.
What is especially notable is that newer agents such as CagriSema and retatrutide were not developed from internet hype or isolated animal papers. They came out of deliberate attempts to improve on already successful incretin therapies by combining or expanding validated hormone pathways. That makes the whole class fundamentally different from what is typically seen with many unapproved peptides.
Summary Of Human Studies
Human data for semaglutide and tirzepatide are robust and clinically important. These drugs have demonstrated meaningful weight loss, improved glycemic control, and broader cardiometabolic benefit in large phase 3 programs and subsequent regulatory review. Semaglutide and tirzepatide are already established as highly effective obesity therapies, and their benefits go well beyond a few pounds of fat loss. Tirzepatide also achieved FDA approval for obstructive sleep apnea in adults with obesity, which highlights how clinically meaningful the weight loss and metabolic effects can be.
CagriSema and retatrutide are especially interesting because they appear capable of pushing efficacy even further. Novo Nordisk announced that CagriSema was submitted to FDA in December 2025 for weight management based on the REDEFINE 1 and REDEFINE 2 pivotal trials. Lilly announced phase 3 retatrutide results showing average weight loss of 28.7% at 68 weeks in TRIUMPH-4 in obesity with knee osteoarthritis, and another phase 3 result in type 2 diabetes showing A1C reductions of 1.7% to 2.0% with 16.8% average weight loss at the 12 mg dose. Those are very strong signals, although both drugs remain investigational in these settings until regulatory review is complete.
One important issue with incretin therapy is that weight loss is not purely fat loss. A meaningful portion of the weight lost on semaglutide, tirzepatide, and related agents comes from lean mass, which includes muscle. Reviews of body composition studies suggest that fat-free mass loss often accounts for roughly 20% to 40% of total weight lost, although the exact proportion varies by drug, study design, baseline body composition, age, protein intake, and physical activity. That does not mean incretins are bad drugs. They are clearly highly effective and can produce major health benefits. But it does mean patients should not assume every pound lost is fat. This is especially important in older adults, patients with low baseline muscle mass, and anyone at risk for sarcopenia. In practice, the best way to reduce muscle loss during incretin therapy is to combine the medication with resistance training, adequate protein intake, and ongoing attention to strength and physical function rather than focusing on the scale alone. There are ongoing studies considering the impact of muscle anabolic agents to prevent the loss in muscle mass, but this is an emerging area.
FDA Approval Status
Semaglutide is FDA approved in the United States, including Wegovy for chronic weight management and other approved indications, and Ozempic for type 2 diabetes. Tirzepatide is FDA approved as Mounjaro for type 2 diabetes and as Zepbound for chronic weight management, with an additional FDA approval for moderate to severe obstructive sleep apnea in adults with obesity. CagriSema is not yet FDA approved, but it has been submitted to FDA for weight management. Retatrutide is not FDA approved and remains in phase 3 development.
Alternatives
The more practical clinical question is which incretin is the best fit for the patient and whether an incretin is appropriate at all. In patients with obesity, type 2 diabetes, OSA related to obesity, or MASH, these drugs may be among the most effective medical options currently available. CagriSema and retatrutide are especially promising, but until they receive approval they should still be viewed as investigational rather than established therapies. There are also previous generations of incretins, such as dulaglutide (Trulicity) and liraglutide (Victoza/Saxenda) that still have clinical utility in treating obesity and diabetes, but their use is declining as they are generally less effective than
Ipamorelin
Brief Background
Ipamorelin is a pentapeptide that is marketed online as a growth hormone secretagogue. It became popular because it is often presented as a "cleaner" or more selective way to increase growth hormone compared with other peptides in the same general category. In wellness and performance circles, it is commonly promoted for increasing lean mass, improving recovery, reducing fat, and helping people eat more by increasing appetite. It is also often paired with CJC-1295 in anti-aging and body composition protocols.
Part of the appeal of ipamorelin is that it sounds more refined than many other peptides. It is often described as selective, physiologic, and lower risk. But that online framing is much more reassuring than the actual evidence base. Human clinical data are limited, most of the hype around the peptide has been built on theory and extrapolation, and there are real concerns about long term endocrine and metabolic effects that are rarely acknowledged in social media discussions.
How The Peptide Is Thought To Work
Ipamorelin works by activating the ghrelin or growth hormone secretagogue receptor, also called GHSR1. This stimulates the pituitary gland to release growth hormone in a pulsatile manner. Unlike some other growth hormone secretagogues, ipamorelin appears to have less effect on cortisol and prolactin release, which is one reason it has been marketed as a more selective option.
That said, activating the ghrelin receptor does not only affect growth hormone. Ghrelin signaling is involved in appetite regulation, glucose metabolism, and broader neuroendocrine physiology. This is an important point because the online discussion often makes ipamorelin sound like a simple muscle or recovery peptide, when in reality it is acting on a receptor with much broader metabolic consequences. That makes the peptide more biologically active and potentially more complicated than the marketing suggests.
Summary Of In Vitro And Animal Model Studies
Preclinical work suggests ipamorelin can stimulate growth hormone release and may have effects similar to other growth hormone secretagogues in musculoskeletal contexts. Animal studies have shown that it can promote longitudinal bone growth and engage pathways relevant to growth and tissue adaptation. That general biology helps explain why people have become interested in it for recovery, body composition, and muscle related goals.
At the same time, preclinical studies also raise concerns that do not fit neatly with the peptide's online reputation. Ghrelin receptor activation appears to stimulate food intake and adiposity, which cuts against the way ipamorelin is often marketed as a body composition optimization drug. There are also mechanistic concerns around chronic ghrelin pathway activation and its broader endocrine consequences. So even at the preclinical level, the story is more mixed than the wellness space usually admits.
Summary Of Human Studies
Human studies of ipamorelin are limited. One small phase II study looked at a short seven-day course of ipamorelin in patients with postoperative ileus. The drug appeared to be generally safe over that brief time frame, but it did not improve the main clinical outcomes being studied. That is a very thin human evidence base for a peptide that is often marketed as if it is a well-established tool for growth, recovery, and performance.
The larger problem is that short term tolerability is not the same thing as long-term safety. There is still very little human data telling us what chronic or repeated use of ipamorelin does in real world patients. That matters because there are plausible concerns around glucose regulation, insulin sensitivity, appetite signaling, and pituitary biology. It is also worth noting that even though ipamorelin is often promoted for lean mass and performance, there is no strong human clinical literature showing that it safely produces those outcomes in the way people online often imply.
FDA Approval Status
Ipamorelin is not FDA approved. It is also among the peptides that have raised enough concern to be restricted in compounding contexts. That matters because many patients assume that if a peptide is widely sold through clinics or peptide vendors, it must have some degree of legitimacy. That is not true. Availability should not be confused with approval, good evidence, or a well-defined safety profile.
Alternatives
The right alternative depends on the actual goal. If the interest in ipamorelin is really about increasing appetite, the first step is usually nutritional strategy, including more calorie dense foods, meal timing, and addressing the reason appetite is poor in the first place. In selected patients, approved appetite stimulating medications may be more rational than using an unapproved ghrelin receptor agonist.
If the goal is improving body composition, preserving muscle, or recovering after injury, there are much better-established approaches. These include progressive rehabilitation, resistance training, adequate protein intake, sleep optimization, and evidence based medical treatment tailored to the actual problem. If the goal is weight loss or fat reduction, ipamorelin makes even less sense, since ghrelin receptor activation may actually increase hunger and adiposity. In most cases, ipamorelin is better understood as an under-studied endocrine peptide with uncertain long-term consequences than as a well-supported recovery or performance therapy.
Kisspeptin
Brief Background
Kisspeptin is an endogenous peptide that plays a central role in regulating the hypothalamic-pituitary-gonadal axis. It is one of the key upstream signals controlling gonadotropin releasing hormone, and because of that it has attracted major interest in reproductive endocrinology, fertility, hypogonadism, and sexual medicine. In peptide and wellness circles, it is often promoted for libido, sexual desire, testosterone support, and fertility enhancement.
Unlike many gray market peptides, kisspeptin is a scientifically serious molecule with a real translational research program behind it. It is not just a hype driven compound. At the same time, it is still not an FDA approved drug, and most of the current therapeutic enthusiasm is based on early human studies and experimental clinical development rather than established routine use. FDA has specifically listed kisspeptin-10 among compounds that may present significant safety risks in the compounding context because of immunogenicity concerns, peptide impurity issues, and limited safety information for proposed routes of administration.
How The Peptide Is Thought To Work
Kisspeptin works by binding to the KISS1 receptor on neurons that regulate gonadotropin releasing hormone. In practical terms, it acts as a master upstream reproductive signal. Once that pathway is stimulated, downstream effects include increased luteinizing hormone and follicle stimulating hormone release, with secondary effects on sex steroid production and broader reproductive function. This is the core reason kisspeptin has attracted so much interest in both fertility medicine and sexual medicine.
Kisspeptin also appears to have effects beyond classic reproductive hormone release. Human and translational work suggests it may influence sexual and emotional brain processing, which is why it is now being explored not just for fertility or hypogonadism, but also for disorders of sexual desire. That makes it more interesting than a simple testosterone support peptide. It may be acting both through endocrine pathways and through central nervous system circuits relevant to sexual motivation.
Summary Of In Vitro And Animal Model Studies
Preclinical work has strongly established kisspeptin as a fundamental reproductive signaling peptide. Animal studies show that it is deeply involved in puberty, fertility, gonadal regulation, and sexual behavior. That preclinical foundation is unusually strong compared with many peptides discussed online, because kisspeptin is not being reverse engineered from hype. It emerged from serious basic science on reproductive physiology.
Animal and translational studies also support a role for kisspeptin in sexual behavior and in integration of sensory and emotional cues relevant to reproduction. This is one reason the peptide has generated so much excitement in psychosexual medicine. Still, even strong physiology and preclinical work do not automatically establish a drug as ready for broad clinical use. They justify further study, not casual peptide prescribing.
Summary Of Human Studies
Human studies of kisspeptin are encouraging. Clinical and translational studies have shown that kisspeptin administration can stimulate reproductive hormone release in humans, which is why it has been explored for reproductive endocrinology and secondary hypogonadism. More recently, randomized clinical trial data in men with hypoactive sexual desire disorder showed that kisspeptin significantly modulated sexual brain processing and increased sexual behavior and penile tumescence in response to visual sexual stimuli. That is a meaningful signal and one of the more interesting human datasets in peptide based sexual medicine.
At the same time, the human evidence is still early. Kisspeptin has not yet developed the kind of large, mature clinical trial base that would support routine mainstream prescribing across the wide range of uses people discuss online. It is best understood as a promising investigational peptide with real human signal, especially in reproductive and psychosexual medicine, but not yet as an established standard therapy.
FDA Approval Status
Kisspeptin is not FDA approved. FDA has stated that compounded drugs containing kisspeptin-10 may pose risk for immunogenicity for certain routes of administration, may have complexities related to peptide impurities and active pharmaceutical ingredient characterization, and that the agency has only limited safety information for proposed routes of administration.
Alternatives
The right alternative depends on the clinical goal. If the goal is treatment of hypogonadism or fertility related dysfunction, the better supported options are standard endocrine and reproductive therapies tailored to the actual diagnosis, such as clomiphene, enclomiphene, hCG, gonadotropins, or testosterone in the appropriate clinical setting. If the goal is sexual desire or psychosexual dysfunction, the more rational approach is to define the problem first and then use evidence based sexual medicine, mental health, and endocrine strategies rather than jumping immediately to an investigational peptide.
The broader point is that kisspeptin is one of the more promising research peptides because the biology is real and the early human data are encouraging. But it is still an unapproved peptide, and most patients do not need an experimental reproductive neuropeptide when better characterized options already exist for the main problems they are trying to solve.
KPV (lysine-proline-valine)
Brief Background
KPV is a short tripeptide of lysine-proline-valine derived from the C-terminal region of alpha melanocyte stimulating hormone (α-MSH). It has attracted attention because it is promoted as an anti-inflammatory peptide, especially for gut inflammation, skin inflammation, wound healing, and various chronic inflammatory conditions. In online peptide culture, KPV is often presented as a smaller and supposedly safer derivative of a naturally occurring signaling peptide, which makes it sound simple and low risk.
The problem is that KPV is still an unapproved peptide with a much thinner human evidence base than the marketing usually suggests. It is biologically interesting, and there is a real preclinical literature behind it, especially in inflammatory bowel disease models. But that is very different from saying it is an established therapy for colitis, skin disease, or systemic inflammation in humans.
How The Peptide Is Thought To Work
KPV is thought to work through anti-inflammatory melanocortin related pathways. It appears to reduce inflammatory signaling and cytokine activity, and some work suggests its effects may involve melanocortin receptor biology, especially MC3R related mechanisms. In the gut, another important part of the story is that KPV can be transported through the PepT1 peptide transporter, which may help explain why it has shown activity in intestinal inflammation models.
That mechanism makes biologic sense, especially for diseases where excessive immune activation and epithelial injury are central problems. But once again, a coherent mechanism is not the same thing as proven clinical efficacy. Anti-inflammatory signaling can look very promising in laboratory systems and animal disease models, yet still fail to become a useful or scalable treatment in people.
Summary Of In Vitro And Animal Model Studies
Preclinical studies are the main reason KPV continues to attract interest. Laboratory and animal work suggests that KPV can reduce intestinal inflammation, improve epithelial healing, and lessen inflammatory injury in colitis models. Some studies have shown that PepT1 mediated uptake of KPV reduces intestinal inflammatory responses, while others suggest it may help in models of colitis associated cancer by reducing inflammatory burden. There is also interest in skin and wound related applications, although the strongest preclinical story appears to be in intestinal inflammation.
These findings are encouraging, but they are still preclinical. A peptide that looks useful in cells grown in a dish or injected into rodent colons is not automatically ready for routine clinical use. The gap between mechanistic promise and real-world human treatment is especially important in inflammatory disease, where many compounds show early signal and then fail when studied properly in patients.
Summary Of Human Studies
Human studies of KPV appear to be extremely limited. Most of the published literature centers on mechanistic work, animal models, and experimental delivery systems rather than on robust human therapeutic trials. That is a major limitation, because KPV is often discussed online as if it is already a practical anti-inflammatory treatment, but in reality the human evidence base does not support that level of confidence.
At this point, there is not a meaningful body of human clinical trial data showing that KPV safely and effectively treats inflammatory bowel disease, skin inflammation, or broader inflammatory syndromes in the way it is often marketed. It is better understood as an interesting experimental anti-inflammatory peptide than as a clinically established therapy.
FDA Approval Status
KPV is not FDA approved. FDA's September 2024 update for bulk drug substances nominated for compounding under section 503A lists KPV in Category 2, meaning it is considered among the substances that raise significant safety risks in the compounding context.
Alternatives
If the goal is inflammatory bowel disease care, there are far better characterized and approved therapies, including mesalamine, corticosteroids, immunomodulators, and biologics depending on disease severity and phenotype. If the goal is skin inflammation, the more rational approach is to identify the diagnosis first and then use evidence based dermatologic treatment rather than an experimental peptide.
The broader point is that for most of the outcomes people hope to get from KPV, there are already approved anti-inflammatory therapies with a much clearer idea of how they work, what the safety profile looks like, and how they perform in real patients. KPV may remain scientifically interesting, but that is not the same thing as being ready for real world clinical use.
Melanotan II
Brief Background
Melanotan II is a synthetic melanocortin peptide that became popular online as an injectable or intranasal "tanning peptide." It is marketed for skin darkening, reduced need for UV exposure, and sometimes for libido or erectile effects. A major source of confusion is that people often mix up Melanotan II with afamelanotide, which is a different melanocortin analog that is used medically in a specific rare condition. Melanotan II itself is unlicensed, largely untested for routine consumer use, and widely sold through gray market channels rather than through standard medical pathways.
Part of the appeal of Melanotan II is obvious. It promises a tan without the same amount of sun exposure, and it sits at the intersection of aesthetics, sexuality, and peptide culture. But this is another peptide where the online conversation is much more casual than the actual risk profile justifies. It has been associated with nausea, flushing, yawning, spontaneous erections, priapism, kidney complications, and other adverse effects, and it is not an FDA approved consumer tanning drug.
How The Peptide Is Thought To Work
Melanotan II works by activating melanocortin receptors, especially MC1R on melanocytes, which increases eumelanin production and darkens the skin. It also has activity at other melanocortin receptors, which helps explain why it can have effects beyond pigmentation, including nausea, appetite related effects, and sexual side effects such as increased erections in some users.
That broader receptor activity is an important reason to be cautious. Online it is often sold as if it is simply a "tanning peptide," but it is really a neuroactive and hormonally active melanocortin agonist with effects that extend well beyond skin pigmentation. That makes it much more biologically active, and potentially much less predictable, than the marketing suggests.
Summary Of In Vitro And Animal Model Studies
The biologic rationale for Melanotan II comes from melanocortin pathway research showing that melanocortin agonists can stimulate pigmentation and affect sexual and central nervous system pathways. That preclinical biology is strong enough to explain why the compound darkens skin and why it was studied in erectile dysfunction and related areas.
But having a clear biologic effect is not the same thing as being a good drug for routine consumer use. Melanotan is not a case where the mechanism is uncertain. The problem is that the real-world safety profile, product quality, and risk-benefit balance are not reassuring enough to support casual use, especially when products are sourced from the gray market.
Summary Of Human Studies
Human studies do show that Melanotan II can increase pigmentation. Early clinical work demonstrated tanning effects in humans after a small number of low dose injections, and other human studies explored erectile effects because melanocortin agonists can trigger erections through central pathways.
The problem is that the human literature also includes meaningful adverse events and case reports that are hard to ignore. Published reports describe systemic toxicity with sympathomimetic type symptoms, rhabdomyolysis (muscle breakdown), renal dysfunction, kidney failure, priapism (erections that don't go away), and concerning pigmentary or melanoma-associated presentations. That does not prove every user will have a serious event, but it does make it very hard to justify the relaxed way the drug is discussed online.
FDA Approval Status
Melanotan II is not FDA approved. FDA previously warned that Melanotan II was being illegally marketed as a new drug without an approved application, and regulators in other countries have also warned consumers against melanotan products sold online. In practical terms, Melanotan II should be viewed as an unapproved gray market peptide, not as a legitimate mainstream therapeutic product.
Alternatives
If the goal is cosmetic tanning, the safer alternative is not another peptide. It is topical sunless tanning products, cosmetic bronzing products, and better skin protection habits. If the goal is to reduce UV damage while improving appearance, a much more rational approach is sun protection, self-tanners, and dermatologic skin care rather than an unapproved injectable melanocortin agonist.
If the interest in Melanotan is partly driven by libido or erectile effects, there are much better studied and safer options depending on the actual problem. These may include tadalafil or sildenafil for erectile dysfunction, PT-141, or a broader sexual medicine evaluation if the issue is more complex. The main point is that there are safer and better characterized alternatives than using an unapproved peptide that affects both pigmentation and multiple other biologic systems.
MOTS-c
Brief Background
MOTS-c (Mitochondrial Open Reading Frame of the 12S rRNA type-c) is a mitochondrial derived peptide that has attracted a lot of attention because it is marketed as an "exercise mimetic." In wellness and performance circles, it is commonly promoted for fat loss, improved insulin sensitivity, better endurance, and increased metabolic efficiency. The idea that a peptide could mimic some of the beneficial effects of exercise is obviously attractive, especially to people looking for shortcuts to better body composition or athletic performance.
Part of the appeal of MOTS-c is that it sounds modern and scientifically sophisticated. It is tied to mitochondria, metabolism, and exercise biology, which makes it especially easy to market online. But the reality is that MOTS-c remains much more interesting scientifically than it is clinically useful at this point. Most of the excitement around the peptide comes from preclinical work and biologic theory, not from strong human therapeutic data.
How The Peptide Is Thought To Work
MOTS-c is thought to work through effects on metabolic signaling pathways, especially pathways involving AMPK and the folate cycle. In practical terms, it appears to shift cells toward improved glucose handling, greater fatty acid oxidation, and broader metabolic adaptation under stress. That is why it is often described as a peptide that may mimic some aspects of exercise or improve metabolic resilience.
The problem is that manipulating these pathways is not necessarily simple or risk free. AMPK signaling, folate metabolism, and nucleotide biosynthesis are fundamental biologic processes. A compound that alters those systems may potentially have useful metabolic effects, but it may also create unintended consequences if pushed chronically or outside the settings in which it has been carefully studied. That is one reason MOTS-c should not be treated like a casual wellness peptide.
Summary Of In Vitro And Animal Model Studies
Preclinical studies in animals are the main reason MOTS-c became popular. In animal models, MOTS-c has been reported to prevent diet induced obesity, improve insulin sensitivity, and support metabolic homeostasis. These findings are the basis for much of the online excitement around the peptide. The preclinical story is one of improved metabolic efficiency, better fuel handling, and possible exercise mimetic effects.
These are interesting findings, but they need to be interpreted carefully. Many compounds look impressive in rodent models and never become useful human therapies. This is especially true for metabolic diseases -- obesity and diabetes have been "cured" many times in mice and rats, but this has not directly translated to a consistent cure in humans. It is especially easy for animal studies in this space to get overinterpreted, because improvements in weight gain or insulin signaling in mice can sound very compelling in a marketing context. That does not mean the same effect will hold up safely or meaningfully in real patients.
Summary Of Human Studies
Human data on MOTS-c are very limited. The main human literature consists largely of observational work looking at endogenous MOTS-c levels and how those levels correlate with insulin sensitivity or other metabolic traits. That is very different from demonstrating that giving MOTS-c to people as a therapy is safe and effective. Correlation studies may be biologically interesting, but they do not establish MOTS-c as a clinically useful drug.
At this point, there is not a meaningful body of human clinical trial data showing that MOTS-c safely improves athletic performance, increases energy, reduces body fat, or treats insulin resistance in the way it is often marketed online. That gap is important. MOTS-c is often discussed as if it is already a legitimate metabolic therapy, but right now the human evidence does not support that level of confidence.
FDA Approval Status
MOTS-c is not FDA approved. It has not established the kind of human safety and efficacy profile that would justify routine clinical use, and it remains much more of an experimental peptide than a legitimate medical therapy.
Alternatives
The right alternative depends on the actual goal. If the goal is weight loss, there are approved and much better studied options such as GLP-1 receptor agonists and phentermine. If the goal is improving insulin sensitivity, there are several evidence-based therapies including metformin, GLP-1 based therapies, SGLT2 inhibitors, and thiazolidinediones. If the goal is athletic performance or increased energy, the more rational approach is usually to optimize sleep, training, carbohydrate availability, iron status when indicated, and proven ergogenic aids such as creatine and caffeine.
The broader point is that for most of the outcomes people hope to get from MOTS-c, there are already approved or much better characterized treatments available. MOTS-c may remain scientifically interesting, but that is not the same thing as being ready for real world clinical use.
Oxytocin
Brief Background
Oxytocin is an endogenous neuropeptide best known for its roles in labor, lactation, bonding, and social behavior. It also has important effects on sexual arousal, orgasm, pair bonding, autonomic tone, and pelvic floor related physiology, which is why it has attracted interest in sexual medicine and pelvic health. In wellness and peptide spaces, oxytocin is often marketed for libido, intimacy, orgasm, erectile function, pelvic pain, and relational connection. That broad appeal makes sense biologically, but it also means the peptide is often marketed much more confidently than the clinical evidence would justify.
Oxytocin is different from many gray market peptides because it is a real endogenous signaling molecule with a long physiologic literature behind it. But that should not be confused with proof that intranasal or compounded oxytocin is an established treatment for pelvic pain or sexual dysfunction. In these areas, the clinical story is still mixed and much less mature than the online conversation usually suggests.
How The Peptide Is Thought To Work
Oxytocin is thought to work through oxytocin receptors in the brain, spinal cord, reproductive tract, pelvic organs, and peripheral tissues. In practical terms, it appears capable of influencing sexual motivation, orgasmic processing, pelvic smooth muscle behavior, stress responsivity, and social-emotional context. That makes it a plausible peptide for both sexual health and selected pelvic pain presentations, especially when pain and sexual symptoms are closely linked with autonomic arousal, guarding, relationship stress, or pelvic floor overactivity. Oxytocin also appears to reduce pain sensation at the level of the spinal cord.
The mechanism is attractive, but it is also one reason oxytocin is easy to oversell. Sexual function and pelvic pain are heavily shaped by context, expectation, relationship factors, mood, and central nervous system processing. That means a peptide with plausible central effects can generate enthusiasm long before it proves itself in rigorous trials. This is especially important in female sexual dysfunction, where placebo responses are very large.
Summary Of In Vitro And Animal Model Studies
Preclinical work strongly supports a role for oxytocin in sexual behavior, partner bonding, reproductive signaling, and stress regulation. Animal studies suggest oxytocin receptor activity in key hypothalamic and limbic regions is linked to sexual experience and sexual reward processing, which provides a coherent biologic basis for why oxytocin might affect arousal, orgasm, and aspects of pelvic function.
That said, strong physiologic relevance is not the same thing as a reliable drug effect in clinical practice. Many pathways involved in sexual behavior and pain modulation are real and important, but translating them into a reproducible treatment is much harder than simply showing the system matters biologically. That is where the clinical literature on oxytocin remains much more modest than the mechanistic story.
Summary Of Human Studies
Human studies on oxytocin for sexual health are mixed. Some studies suggest possible effects on orgasm intensity, erectile function, post-sexual contentment, or related subjective domains. But this is not the same thing as having a large, convincing clinical trial base. For pelvic pain specifically, direct human evidence is limited. The rationale is stronger than the proof. Oxytocin may eventually find a role in carefully selected patients whose pelvic pain overlaps with sexual dysfunction, pelvic floor tension, or central-autonomic dysregulation, but it should be carefully evaluated when considering off-label use.
FDA Approval Status
Oxytocin is FDA approved as an injection for obstetric indications such as induction or augmentation of labor and control of postpartum uterine bleeding. Its use for sexual health is off-label.
Alternatives
The right alternative depends on the actual problem being treated. If the goal is erectile function, PDE5 inhibitors such as tadalafil or sildenafil could be helpful, along with a broader evaluation of vascular, hormonal, pelvic floor, and psychosexual contributors. If the goal is low sexual desire, the treatment depends on sex, hormonal status, and the broader clinical picture, but may include relationship work, psychosexual therapy, hormone therapy when indicated, or approved therapies such as PT-141/bremelanotide in the appropriate population. For pelvic pain, the alternatives are usually much more diagnosis specific and may include pelvic floor physical therapy, downtraining, bowel and bladder management, neuromodulation, tadalafil in selected pelvic pain syndromes. Oxytocin may have a role as a supplemental treatment to pain syndromes and erectile dysfunction, rather than a replacement for traditional treatments.
PT-141/Bremelanotide
Brief Background
PT-141 is the developmental name for bremelanotide, a melanocortin receptor agonist that works very differently from the PDE5 inhibitors Viagra and Cialis. Instead of acting mainly through penile or clitoral blood vessel smooth muscle, PT-141 works centrally through melanocortin pathways involved in sexual arousal and desire. That difference is important because it helps explain why PT-141 drew so much interest as a potential treatment not only for erectile dysfunction, but also for sexual desire disorders. It is now FDA approved as Vyleesi for acquired, generalized hypoactive sexual desire disorder in premenopausal women. Vyleesi is specifically not indicated for men under the approved labeling, although the clinical trials data in men demonstrate favorable findings.
PT-141 is one of the more interesting peptides in sexual medicine because the clinical data are genuinely encouraging. In women, PT-141 went through the modern approval pathway and demonstrated enough efficacy and safety for FDA approval in a clearly defined indication. In men, the data are also quite promising, particularly in erectile dysfunction and in men who have not responded adequately to sildenafil. PT-141 never completed the regulatory path to male approval, even though the biologic rationale and early clinical signal were both strong. Nausea is a common occurrence, with up to 20% of patients experience this side effect.
How The Peptide Is Thought To Work
PT-141 is a nonselective melanocortin receptor agonist, with clinically relevant activity at melanocortin receptors involved in central nervous system sexual signaling. In simple terms, it acts upstream of erection and arousal by engaging brain pathways that influence sexual desire and erectile response. That makes it fundamentally different from drugs like sildenafil and tadalafil, which mainly improve the vascular mechanics of erection by preserving nitric oxide mediated smooth muscle relaxation.
This difference is one reason PT-141 has remained clinically attractive. Because it acts centrally, it may help some patients whose sexual dysfunction is not purely a blood flow problem. That includes women with low desire and men whose erectile dysfunction involves more than simple penile vascular impairment. It also helps explain why PT-141 has shown signal in men who did not respond adequately to PDE5 inhibitors alone. Rather than replacing those drugs mechanistically, it may complement them.
Summary Of In Vitro And Animal Model Studies
The biologic rationale for PT-141 is strong. Melanocortin signaling has long been linked to erection, arousal, and sexual behavior in preclinical models, which is why melanocortin agonists became an area of interest in both male and female sexual dysfunction. PT-141 emerged from that line of work as a compound with clear erectogenic and prosexual effects that did not rely on the same peripheral vascular mechanism as PDE5 inhibitors.
That preclinical foundation is stronger than what exists for many peptides discussed online because the peptide's core effect on sexual physiology is not vague or speculative. It is supported by a coherent receptor-based mechanism and by translational work that makes sense biologically. This is one reason PT-141 should be viewed very differently from hype driven peptides that have little more than animal injury data and testimonials behind them.
Summary Of Human Studies
The human data in women are encouraging enough that PT-141 achieved FDA approval for premenopausal women with acquired, generalized hypoactive sexual desire disorder. In the phase 3 RECONNECT studies, PT-141 improved sexual desire and reduced related distress compared with placebo, and longer-term extension data supported a generally manageable safety profile. That does not make it a miracle drug, but it is a real medication with real phase 3 data and a real regulatory approval in women.
The human data in men are also encouraging. Early randomized trials showed erectogenic effects in men with erectile dysfunction, including men who had not responded adequately to sildenafil. In one randomized controlled study, intranasal bremelanotide improved erectile responses in sildenafil nonresponders, and combination work also suggested that low dose PT-141 plus sildenafil could outperform sildenafil alone. Reviews of emerging ED therapies continue to describe bremelanotide as a promising option for male ED, especially as an adjunct or salvage strategy. The biggest limitation was not lack of signal. It was tolerability and hemodynamic concern at the highest doses. The blood pressure effects appear to be transient, but potentially concerning in a male with existing hypertension.
FDA Approval Status
PT-141, as bremelanotide injection marketed as Vyleesi, is FDA approved for acquired, generalized hypoactive sexual desire disorder in premenopausal women. The approved labeling specifically states that it is not indicated for postmenopausal women, not indicated for men, and not indicated to enhance sexual performance. That means PT-141 has a legitimate FDA approved use, but post-menopausal female or male use remains off label and outside the approved indication.
Alternatives
The more useful clinical comparison is with other sexual medicine therapies. In men with erectile dysfunction, PDE5 inhibitors remain first line because they are easy to use, effective for many patients, and well established. PT-141 is potentially most interesting in men who do not respond adequately to PDE5 inhibitors alone, in men whose dysfunction is not purely vascular, or in patients where a centrally acting approach may be useful.
In women with low desire, PT-141 is now one of the few legitimate prescription options with FDA approval in a defined population. That alone makes it very different from most peptides discussed in online wellness culture.
Selank
Brief Background
Selank is a synthetic heptapeptide derived from tuftsin, an endogenous immunomodulatory peptide. Developed in Russia in the 1980s and 1990s, selank is most often marketed for anxiety, stress resilience, mood, focus, and "nootropic" effects. In online peptide culture, it is commonly framed as a calmer, safer, non-benzodiazepine way to improve anxiety and cognitive function, usually as an intranasal product. Most of the literature behind selank comes from Russian-language or Russia-linked research, and the human evidence base is much smaller and much less internationally validated than the online discussion usually suggests.
Part of the appeal of selank is that it sits at the intersection of psychiatry, cognitive enhancement, and peptide culture. That makes it especially easy to hype online. But it is still an experimental neuroactive peptide in the US context, not an established mainstream treatment for anxiety or cognitive complaints. Its regulatory status, manufacturing concerns, and limited high quality human data all matter here.
How The Peptide Is Thought To Work
Selank is thought to work through effects on GABA related neurotransmission and broader modulation of monoamine and neuroimmune signaling. Preclinical mechanistic studies suggest it may act as a positive allosteric modulator of GABA receptor related activity and may also alter expression of genes involved in neurotransmission. This is the biologic basis for claims that it may reduce anxiety while avoiding the sedation and dependency profile people associate with benzodiazepines.
That said, a plausible neurobiologic mechanism is not the same thing as proven clinical utility. Neuroactive peptides are especially vulnerable to overinterpretation because changes in anxiety, calmness, and focus are subjective, expectancy-sensitive outcomes. That makes it easy for a compound with an interesting mechanism to get far ahead of its actual human evidence base, especially when it is marketed through clinics and online communities that emphasize benefits and rarely discuss uncertainty.
Summary Of In Vitro And Animal Model Studies
Preclinical studies suggest selank may have anxiolytic, anti-stress, and cognitive effects in laboratory and animal settings. Experimental work has reported changes in gene expression related to neurotransmission, effects on GABA related signaling, and anxiety-reducing or cognition-supporting effects in rodent stress models. These kinds of data help explain why selank became popular as a "brain peptide".
But as with many peptides, the preclinical story is more mature than the clinical one. Animal models of anxiety and cognition can generate interesting hypotheses, but they do not establish that a peptide safely and meaningfully improves real world anxiety disorders, attention problems, or performance in humans. That gap is especially important for a peptide being used in otherwise healthy people for wellness or enhancement purposes.
Summary Of Human Studies
Human studies on selank are limited and relatively small. Published reports describe anxiolytic effects in generalized anxiety disorder and suggest possible cognitive or tolerability advantages compared with standard anxiolytics in some settings, but these data are not the same as a large, independently replicated international evidence base. The studies most often cited are small and come from a narrow, foreign literature stream, which makes it harder to know how well the findings generalize.
So the human evidence is not absent, but it is still much thinner than the marketing usually implies. Selank should not be treated as if it has the same validation as standard psychiatric medications or mainstream evidence-based anxiety treatments. At this point, it is better understood as an experimental neuroactive peptide with some early human signals than as an established clinical therapy.
FDA Approval Status
Selank is not FDA approved. FDA has also stated that compounded drugs containing selank may pose risk for immunogenicity for certain routes of administration because of the potential for aggregation and peptide related impurities, and the agency says it lacks important information regarding safety issues raised by selank administered to humans.
Alternatives
If the goal is treatment of anxiety, safer and more evidence based alternatives include cognitive behavioral therapy, exposure based therapy when indicated, limited SSRIs or SNRIs, buspirone, and in selected cases short term use of standard anxiolytics. If the goal is better focus, stress resilience, or cognitive performance, the first step is usually not a peptide. It is sleep optimization, treatment of anxiety or depression if present, evaluation for ADHD when appropriate, and careful attention to caffeine use, exercise, and overall recovery. These approaches are far better characterized than selank and have much clearer real-world evidence behind them.
Semax
Brief Background
Semax is a synthetic peptide derived from adrenocorticotropic hormone fragments and is most often discussed as a nootropic or neuroprotective peptide. It is commonly marketed for focus, cognition, recovery from stress, and sometimes stroke or brain injury support. Part of the appeal of semax is that it sounds more sophisticated and less risky than traditional psychiatric or neurologic medications. It is often framed online as a peptide that can improve mental performance without the tradeoffs of standard drugs. But the clinical literature is limited, much of it comes from a relatively narrow Eastern European research stream, and the level of evidence is nowhere near what most patients would assume based on how confidently the peptide is promoted online.
How The Peptide Is Thought To Work
Semax is thought to influence central nervous system signaling through multiple pathways, including effects on neurotrophic factors such as BDNF, serotonergic systems, and gene expression related to inflammation, vascular biology, and neuroprotection. This is the biologic rationale for why it has been studied in ischemic brain injury, cognitive recovery, and stress related conditions.
That said, a broad and interesting CNS mechanism does not automatically translate into reliable clinical benefits. Neuroactive peptides are especially easy to overmarket because outcomes like focus, calmness, recovery, and cognition are subjective and expectation-sensitive. That means peptides like semax can look more impressive in real world anecdotes than they actually are when studied rigorously.
Summary Of In Vitro And Animal Model Studies
Preclinical studies suggest semax may have neuroprotective, anti-inflammatory, and gene regulatory effects in brain injury models. Laboratory and animal work has reported effects on genes involved in vascular function and neural recovery, and other studies suggest possible modulation of BDNF and related pathways in the brain. These findings help explain why the peptide has been discussed for stroke, hypoxia, and cognitive support.
These kinds of preclinical data are interesting, but they should be interpreted carefully. Many compounds show promising neuroprotective or cognition related signals in animal models and never become useful mainstream human therapies. The fact that semax has mechanistic and animal data does not mean it is established for cognitive enhancement, mental performance, or recovery in otherwise healthy people.
Summary Of Human Studies
Human studies of semax do exist, but the literature is limited and focused largely on neurologic indications such as ischemic stroke rather than on healthy adults seeking better focus or productivity. Reviews from the cognition and aging space note that semax has been used clinically in Russia for stroke, but they also emphasize that there is little evidence for cognitive enhancement in healthy people and no evidence for Alzheimer’s disease.
So while semax is not a completely evidence-free peptide, the human evidence is much narrower than the online hype suggests. It is more accurate to describe it as an experimental neuroactive peptide with some limited clinical history in specific settings than as a proven nootropic or performance enhancer for routine use.
FDA Approval Status
Semax is not FDA approved. FDA has also cited semax as a bulk drug substance used in compounded products that do not qualify for the exemptions under section 503A because it is not the subject of an applicable USP or NF monograph, is not a component of an FDA-approved human drug, and does not appear on the 503A bulks list.
Alternatives
If the goal is treatment of anxiety, attention problems, or cognitive symptoms, the better approach is to first define the real problem. For anxiety, evidence-based options include cognitive behavioral therapy, SSRIs, SNRIs, buspirone, and other standard treatments depending on the clinical picture. For focus or daytime cognitive complaints, the first step is often sleep optimization, evaluation for ADHD when appropriate, management of depression or anxiety if present, and review of caffeine use, exercise, and recovery. In other words, semax is not usually the most rational first move when safer and better characterized alternatives already exist.
Sermorelin And Tesamorelin
Brief Background
Sermorelin and tesamorelin are growth hormone releasing hormone related peptides. They work by stimulating the pituitary gland to release more growth hormone, which then increases IGF-1 production downstream. Tesamorelin is an approved drug for reduction of excess visceral fat in selected patients with HIV associated lipodystrophy. Sermorelin has a more complex regulatory history, but unlike many gray market peptides, it has real human clinical data, a known mechanism, and a much more predictable safety profile than most of the peptides hyped online.
These peptides are not magic recovery drugs, but they are in a different category than many internet peptides. They stimulate the growth hormone axis in a more physiologic way than injecting growth hormone directly. Human studies show some meaningful effects on body composition, especially visceral fat reduction with tesamorelin in patients who are HIV+ and on antiviral medication. In patients who are HIV-, the effects appear to be much less pronounced. Overall fat loss is generally modest, often on the order of a few pounds. When that fat is clinging to the organs, so called visceral fat, losing a few pounds can still result in serious improvements to health. But as a general weight loss tool, where the goal is losing 10 or more pounds of body fat, these peptides are not particularly effective.
How The Peptides Work
Sermorelin is a synthetic fragment of growth hormone releasing hormone, while tesamorelin is a modified full length growth hormone releasing hormone analog with improved stability and potency. Both work by binding to growth hormone releasing hormone receptors in the pituitary gland, which stimulates the physiologic release of growth hormone. That rise in growth hormone then leads to increased IGF-1 production. Because they stimulate the body's own axis instead of replacing growth hormone directly, they are often viewed as a more physiologic way to increase growth hormone signaling.
That does not mean they are risk free or that they should be treated like anti-aging shortcuts. Raising growth hormone and IGF-1 can have real endocrine and metabolic effects. These peptides need proper medical evaluation, appropriate dosing, and monitoring for side effects such as facial flushing, headache, dizziness, fluid related symptoms, hypoglycemia, and glucose related changes. Extensive lab work needs to be performed before they can safely be used. Their safety profile is much better characterized than that of most unapproved peptides, but they still need to be approached like real drugs, not wellness hacks.
Summary Of In Vitro And Animal Model Studies
There is not nearly as much direct preclinical work on sermorelin and tesamorelin in musculoskeletal healing as there is for some of the more heavily hyped gray market peptides. Instead, much of the rationale comes from what is known more broadly about growth hormone and IGF-1 biology. Growth hormone signaling appears to support connective tissue collagen synthesis, and IGF-1 signaling is clearly important for muscle and tendon adaptation, repair, and maintenance. That creates a reasonable biologic basis for why these peptides might help in settings involving disuse atrophy, connective tissue healing, or recovery after injury.
At the same time, biologic rationale should not be overstated. Increasing growth hormone signaling does not automatically translate into major improvements in muscle mass, athletic performance, or faster healing in otherwise healthy adults. The preclinical and mechanistic data support the idea that these peptides may help preserve tissue or support selected repair processes, but they do not justify the much broader claims often made online.
Summary Of Human Studies
Human studies show that tesamorelin can reduce visceral fat in patients with HIV associated lipodystrophy, and this is the setting where the clinical evidence is strongest. There are also data showing that tesamorelin can reduce trunk fat and waist circumference while modestly increasing lean mass. In HIV- patients with reduced growth hormone secretion and obesity, the effects are smaller and much less dramatic than what people often imagine when they hear these drugs discussed online. These are not highly effective weight loss drugs in the usual sense. They can improve body composition in selected settings, but they are not comparable to GLP-1 receptor agonists for general body fat reduction.
Sermorelin has also been studied in humans, and the data suggest it can increase endogenous growth hormone secretion, especially nocturnal growth hormone release, but body composition effects are generally modest. In otherwise healthy adults, increasing growth hormone levels does not appear to meaningfully improve muscle mass or performance. Where this class may be more interesting is in protecting against muscle loss during periods of injury, inactivity, or recovery, and possibly in supporting connective tissue biology in selected settings. There is some rationale for short term use in situations such as ACL injury, tendon injury, or other conditions involving disuse atrophy, but the clinical studies in these areas are still limited and generally small. These are not indications that have been thoroughly established.
One practical issue with tesamorelin is stability after reconstitution. Traditional formulations required rapid use after mixing with sterile water because the peptide degrades relatively quickly in solution. That matters because even when a peptide itself is legitimate, formulation and handling still affect how reliably it performs. This is one reason a gray market version or a poorly prepared compounded version cannot automatically be assumed to behave like a commercial product with controlled manufacturing and formulation.
FDA Approval Status
Tesamorelin is FDA approved for reduction of excess visceral fat in patients with HIV associated lipodystrophy. Sermorelin was previously approved for pediatric growth hormone deficiency related indications and was later discontinued for commercial rather than safety reasons. Its regulatory history is much more legitimate than that of gray market peptides, even though its current status is more complicated than a standard branded drug with a broad commercial presence.
Alternatives
These peptides are not appropriate for most patients whose main goal is general weight loss. For reduction of body fat, especially when the goal is more than a few pounds of fat loss, incretin/GLP-1 receptor agonists such as semaglutide or tirzepatide are much more effective and much better studied. Phentermine may also be useful in selected patients.
SS-31
Brief Background
SS-31, also known as elamipretide or Forzinity, is a short tetrapeptide that has attracted interest because it targets mitochondrial function rather than growth hormone signaling, angiogenesis, or appetite pathways. That alone makes it different from many of the peptides that are heavily promoted online. Instead of being marketed mainly as a healing or body composition peptide, SS-31 has been studied in settings involving mitochondrial dysfunction, fatigue, heart disease, muscle disease, and neurologic injury. It has also been promoted online for endurance, recovery, and performance enhancement, but those claims go well beyond the strongest clinical evidence.
Among peptides discussed in sports medicine and wellness spaces, SS-31 stands out as one of the more scientifically legitimate compounds. It has gone through a much more serious drug development pathway than most gray market peptides, and its safety profile appears more predictable than compounds like BPC-157, CJC-1295, or TB-500. That does not mean it is established for athletic recovery or performance in healthy adults. It is not. But it does mean it belongs in a very different category than the internet peptides that are sold almost entirely on hype.
How The Peptide Is Thought To Work
SS-31 is thought to work by binding selectively to cardiolipin, a phospholipid located in the inner mitochondrial membrane. Cardiolipin is critical for maintaining mitochondrial structure and for efficient function of the electron transport chain, which allows the body to use oxygen to produce energy. By interacting with cardiolipin, SS-31 appears to stabilize mitochondrial membranes, improve electron transport efficiency, and reduce the production of reactive oxygen species, resulting in more energy molecules like ATP and NAD inside of cells.
In practical terms, this means SS-31 is designed to improve mitochondrial energy production and reduce oxidative stress. That mechanism helps explain why researchers have been interested in it for conditions involving impaired cellular energetics, including mitochondrial disorders, heart failure, ischemia-reperfusion injury, and some forms of muscle and neurologic dysfunction. It is a far more targeted and biologically coherent mechanism than the vague "healing" claims that surround many other peptides.
Summary Of In Vitro And Animal Model Studies
Preclinical studies on SS-31 are part of the reason the peptide has generated so much interest. In animal models, SS-31 has shown effects consistent with improved mitochondrial function, reduced oxidative stress, and better cellular energetics. In mouse studies, it improves treadmill endurance and reduce fatigue. In models of traumatic brain injury, it has shown neuroprotective effects linked to reversal of mitochondrial dysfunction. There is also preclinical work suggesting potential benefit in cardiac and skeletal muscle settings where mitochondrial stress is a major part of the disease process.
These animal and mechanistic data are much more coherent than what is seen with many gray market peptides. The preclinical story makes biologic sense. At the same time, even promising mitochondrial biology in animals does not automatically mean SS-31 will improve athletic performance, recovery, or injury healing in otherwise healthy people. That is where online enthusiasm often outruns the science.
Summary Of Human Studies
Human studies of SS-31 are more substantial than those of most unapproved peptides, but they still do not support the broad claims often made online. Clinical development has focused mainly on disease states involving mitochondrial dysfunction rather than on healthy people trying to recover faster or perform better. In human studies, SS-31 has generally been well tolerated and has shown biologic activity consistent with improving mitochondrial function.
One particularly interesting study found that a single infusion improved in vivo mitochondrial ATP production capacity in skeletal muscle in older adults. However, that did not translate into a clear reduction in muscle fatigability in the same study. That distinction matters. Improving a biomarker or a physiologic measurement is not the same thing as producing a meaningful real world change in performance or recovery. While the human data are more serious and more credible than what exists for many peptides, they still do not justify the sweeping performance and recovery claims about SS-31 often made in wellness spaces.
FDA Approval Status
SS-31, under the name elamipretide, is FDA approved for Barth syndrome. This places it in a very different category from most peptides discussed in health and wellness. It is not a gray market-only compound, and it has gone through a formal regulatory review process.
That said, FDA approval in Barth syndrome does not mean SS-31 is approved for athletic performance, general fatigue, injury recovery, or anti aging. Those uses remain outside the approved indication and should not be confused with the much narrower setting in which the drug has actually been studied and authorized.
Alternatives
There are no other approved treatments for Barth syndrome. However, if the goal is better high intensity performance, power output, repeated sprint ability, or strength training quality, the best supported options are still the boring ones: adequate carbohydrate availability, creatine monohydrate, and caffeine. Across recent reviews, creatine remains one of the most consistently supported ergogenic aids for strength, lean mass, and repeated high intensity efforts, while caffeine has some of the strongest evidence for improving exercise performance acutely. If the goal is endurance or training tolerance, the evidence base still favors fundamentals over mitochondria themed compounds sold online. Adequate fueling, especially carbohydrate around training, caffeine in the right setting, and creatine for mixed or repeated high intensity demands are more evidence based than SS-31 for healthy athletes.
Thymosin beta-4 And TB-500
Brief Background
Thymosin beta-4, or Tβ4, is a 43 amino acid peptide that plays a role in cell migration, wound healing, and tissue repair. It is a naturally occurring peptide in the body and has been studied in a range of preclinical and limited human settings. TB-500 is a synthetic fragment derived from the active actin binding region of Tβ4. Online, these two peptides are often discussed almost interchangeably, even though they are not the same molecule and do not have the same evidence base. That distinction matters, because Tβ4 at least has some real experimental and early clinical literature behind it, while TB-500 is much less well characterized.
These peptides became popular because they are marketed as broad healing and recovery agents. In sports performance and regenerative medicine circles, they are often promoted for tendon injuries, muscle injuries, wound healing, recovery after hard training, and general regenerative support. The problem is that the online discussion almost always takes the most optimistic interpretation of the preclinical story and ignores how limited the human evidence actually is. Tβ4 has some real biologic interest, but neither Tβ4 nor TB-500 should be treated like established musculoskeletal therapies.
There are also significant concerns about these peptides in cancer. Tβ4 is overexpressed in multiple tumor types, including colorectal, pancreatic, breast, and lung cancers, and elevated Tβ4 levels correlate with tumor progression, metastasis, and poor prognosis. Tβ4 promotes epithelial-mesenchymal transition, a process important in cancer metastasis, and enhances tumor angiogenesis through the same mechanisms that promote wound healing.
How The Peptides Are Thought To Work
Tβ4 is thought to work mainly through binding and sequestering G-actin, which affects cell migration, cytoskeletal organization, and tissue repair signaling. In practical terms, Tβ4 appears to help coordinate some of the early events involved in wound healing and tissue regeneration. It has also been associated with angiogenesis, inflammatory modulation, and activation of repair related pathways. TB-500 is marketed as a shorter active fragment that supposedly captures some of these same biologic effects, particularly those related to cell migration and healing.
That sounds attractive in a marketing context, but the biology cuts both ways. The same pathways that support wound healing and tissue remodeling can also intersect with tumor biology, angiogenesis, and epithelial-mesenchymal transition. In other words, these are not simple "repair only" peptides. They are biologically active molecules that affect fundamental processes involved in both healing and disease progression. That is one of the most important reasons consumers should be cautious, especially when these compounds are used repeatedly or obtained through gray market channels.
Summary Of In Vitro And Animal Model Studies
Preclinical studies on Tβ4 are the main reason these peptides became popular. In animal models, Tβ4 has been reported to accelerate dermal wound healing, improve collagen organization, reduce scarring, and enhance repair in a variety of injured tissues. In muscle injury models, it appears to act as a chemoattractant for muscle stem cells and may increase regenerating muscle fibers. These kinds of findings make the peptide look highly promising from a regenerative standpoint.
But even the preclinical animal model story needs some restraint. In muscle studies, for example, increases in regenerating fibers did not necessarily translate into improvements in strength. That is an important reminder that tissue level signals do not always turn into meaningful functional outcomes. TB-500 is even more speculative. Much less is known about it, and the literature is far thinner than what exists for full length Tβ4. So while the preclinical data create biologic interest, they do not justify treating these peptides as proven recovery drugs.
Summary Of Human Studies
Human evidence for Tβ4 is limited but not completely absent. Early phase clinical trials have generally suggested that short term use of Tβ4 can be tolerated, and there have been small studies in ophthalmic and cardiovascular settings where it appeared to have some biologic or clinical activity. That is very different from saying it is established for tendon healing, muscle recovery, or athletic performance. Those are exactly the uses that dominate online marketing, and the human literature does not support that level of confidence.
TB-500 is even more problematic because there is very little real human data behind it. Much of what is said online about TB-500 is extrapolated from the biology of Tβ4 or from theoretical claims about the active fragment. That is a weak foundation for clinical decision making. The central issue is that neither peptide has the kind of human outcome literature that would justify routine use for health, wellness, or athletic performance applications, especially when the safety questions remain unresolved.
FDA Approval Status
Tβ4 is not FDA approved for musculoskeletal healing, athletic recovery, or performance enhancement. TB-500 is also not FDA approved. These are not established drugs for the ways they are commonly promoted online, and their availability through peptide vendors or wellness channels should not be confused with legitimacy or good evidence.
Alternatives
The right alternative depends on the actual clinical goal. If the goal is wound healing, soft tissue recovery, or musculoskeletal rehabilitation, the better approach is usually to start with evidence-based treatment specific to the tissue and condition involved. That may include progressive rehabilitation, physical therapy, shockwave therapy, platelet rich plasma, platelet poor plasma, or selected cell-based approaches such as bone marrow aspirate concentrate, microfat, or stromal vascular fraction depending on the indication.
The broader point is that even though Tβ4 and TB-500 are marketed as regenerative shortcuts, there are safer and better characterized ways to approach most of the problems people are trying to solve with them. These peptides are biologically interesting, but the current evidence does not justify the confidence with which they are often sold.
VIP (vasoactive intestinal peptide)
Brief Background
VIP, short for vasoactive intestinal peptide, is an endogenous neuropeptide that is naturally produced in the body. It has broad effects in the nervous system, immune system, lungs, blood vessels, and gastrointestinal tract. Online, VIP is sometimes marketed for chronic inflammatory conditions, fatigue, mold related illness, pulmonary issues, and various poorly defined "recovery" syndromes. That broad marketing reflects how many systems VIP touches biologically, but it also creates a problem because a peptide with wide physiologic actions can be very easy to oversell.
VIP is different from many of the peptides discussed in performance and wellness spaces because it is a real endogenous signaling molecule with a substantial physiologic literature behind it. At the same time, it is not an FDA approved mainstream drug product, and the fact that it is under evaluation in FDA's 503A Category 1 compounding framework should not be mistaken for approval or proof of clinical utility for the many conditions it is promoted for.
How The Peptide Is Thought To Work
VIP works through VPAC receptors and has potent effects on smooth muscle tone, vasodilation, immune signaling, mucus secretion, and airway physiology. In practical terms, it can relax smooth muscle, alter blood flow, and modulate inflammatory responses. That helps explain why it has drawn interest in pulmonary disease and inflammatory conditions.
The problem is that a peptide with this many biologic actions is not simple to use therapeutically. A compound that causes vasodilation and broad immunologic signaling may have plausible benefits in selected settings, but it can also create unwanted systemic effects. That is one reason VIP should not be treated like a casual wellness peptide or a broad-spectrum recovery drug.
Summary Of In Vitro And Animal Model Studies
Preclinical work supports the idea that VIP has anti-inflammatory and bronchodilatory properties, which is why inhaled VIP agonists attracted interest in respiratory therapeutics. Experimental work suggests VIP related signaling may influence airway tone, inflammatory cascades, and tissue responses in the lung. That gives the peptide a more coherent biologic rationale than many gray market compounds that are marketed with little more than vague healing claims.
At the same time, strong endogenous biology and promising preclinical findings do not automatically make VIP a useful real-world treatment for the wide range of disorders it is marketed for online. This is another example of a peptide where mechanistic plausibility can easily outrun practical clinical evidence.
Summary Of Human Studies
Human clinical work on VIP and VIP agonists has been most relevant in pulmonary and respiratory research rather than in the broad chronic illness and wellness settings where the peptide is often promoted. Reviews of inhaled VIP agonists note that several clinical studies have suggested possible therapeutic use in respiratory disease, but this remains a specialized and evolving area rather than a mature, broadly accepted clinical application.
That means VIP is not a completely evidence-free peptide, but the clinical literature does not justify the very broad claims often made online. It is better understood as a biologically interesting peptide with some translational respiratory research than as a proven general treatment for inflammation, fatigue, or complex chronic syndromes.
FDA Approval Status
VIP is not FDA approved as a drug. FDA documents show vasoactive intestinal peptide as a bulk drug substance under evaluation in 503A Category 1, which means it has been nominated with adequate support for evaluation in the compounding framework, not that it has been approved as safe and effective for any clinical indication.
Alternatives
The right alternative depends entirely on the reason someone is interested in VIP. If the goal is treatment of asthma or other airway disease, established inhaled bronchodilators, inhaled corticosteroids, and condition specific pulmonary therapies are much better supported. If the goal is treatment of inflammation, fatigue, or a poorly defined chronic illness syndrome, the better approach is usually to define the actual diagnosis first and then use evidence-based treatment for that condition rather than reaching for a broad acting peptide with limited real world clinical support.
Conclusions

The Bottom Line
Peptides are powerful biologic tools. Some are excellent medicines, while others are experimental compounds that should stay in the research world until proper human data exist. And even for peptides that are truly useful, source quality matters because contamination, degradation, or sequence errors can dramatically change safety and function.
When patients ask about peptides, the first question is not "Which peptide should I take?" It is "What is the real goal?" Weight loss, pain reduction, tendon healing, lean mass, recovery, energy, sexual function, or metabolic improvement all have different evidence-based pathways. Once the goal is clear, it becomes easier to decide whether a peptide belongs in the discussion at all, or whether the safer and better supported answer is something else entirely.
If you are considering peptides for recovery, body composition, or performance, the safest next step is not to order them online. It is to work with a provider who can help you understand what is approved, what is experimental, what is risky, and what evidence-based alternatives may get you where you want to go more safely. We are available as a resource for patients that have questions about peptides, and their safe and appropriate use. Contact us
References
Andia I, Maffulli N. Biological Therapies in Regenerative Sports Medicine. Sports Med. 2017;47:807–28.
Behnia B, Heinrichs M, Bergmann W, et al. Differential effects of intranasal oxytocin on sexual experiences and partner interactions after sexual intercourse in couples. Psychoneuroendocrinology. 2014;45:49-56.
Benedetti F, Mayberg HS, Wager TD, Stohler CS, Zubieta J-K. Neurobiological Mechanisms of the Placebo Effect. J Neurosci. 2005;25:10390–402.
Bes F, Hofman W, Schuur J, van Boxtel CJ. Effects of delta sleep-inducing peptide on sleep of chronic insomniac patients. A double-blind study. Neuropsychobiology. 1992;26(4):193-197.
Bhandarkar A, Bhat S, Kapoor N. Effect of GLP-1 receptor agonists on body composition. Curr Opin Endocrinol Diabetes Obes. 2025;32:279–85.
Burian B, Ortner A, Prassl R, Zimmer A, Mosgoeller W. Clinical potential of VIP by modified pharmaco-kinetics and delivery mechanisms. Endocr Metab Immune Disord Drug Targets. 2012;12(4):344-350.
Carvalho M, Almeida IF. The Role of Pharmaceutical Compounding in Promoting Medication Adherence. Pharmaceuticals. 2022;15:1091.
Chung B, Wiley JP. Extracorporeal Shockwave Therapy. Sports Med. 2002;32:851–65.
Dalmasso G, Charrier-Hisamuddin L, Nguyen HT, et al. PepT1-mediated tripeptide KPV uptake reduces intestinal inflammation. Gastroenterology. 2008;134(1):166-178.
De D, Jamal ME, Aydemir E, Khera A. Social Media Algorithms and Teen Addiction: Neurophysiological Impact and Ethical Considerations. Cureus. 2025;17:e77145.
Diamond LE, Earle DC, Garcia WD, Spana C. Co-administration of low doses of intranasal PT-141, a melanocortin receptor agonist, and sildenafil to men with erectile dysfunction results in an enhanced erectile response. Urology. 2005;65(4):755-759.
Goldstein AL, Hannappel E, Sosne G, Kleinman HK. Thymosin β4: a multi-functional regenerative peptide. Basic properties and clinical applications. Expert Opin Biol Ther. 2012;12:37–51.
González-Sales M, Barrière O, Tremblay PO, Nekka F, Mamputu J-C, Boudreault S, et al. Population pharmacokinetic and pharmacodynamic analysis of tesamorelin in HIV-infected patients and healthy subjects. J Pharmacokinet Pharmacodyn. 2015;42:287–99.
Heffernan M, Summers RJ, Thorburn A, Ogru E, Gianello R, Jiang W-J, et al. The Effects of Human GH and Its Lipolytic Fragment (AOD9604) on Lipid Metabolism Following Chronic Treatment in Obese Mice andβ 3-AR Knock-Out Mice. Endocrinology. 2001;142:5182–9.
Heinemeier KM, Mackey AL, Doessing S, Hansen M, Bayer ML, Nielsen RH, et al. GH/IGF-I axis and matrix adaptation of the musculotendinous tissue to exercise in humans. Scand J Med Sci Sports. 2012;22:e1-7.
Hudgens JL, Sugg KB, Grekin JA, Gumucio JP, Bedi A, Mendias CL. Platelet-Rich Plasma Activates Proinflammatory Signaling Pathways and Induces Oxidative Stress in Tendon Fibroblasts. Am J Sports Med. 2016;44:1931–40.
Ishida J, Saitoh M, Ebner N, Springer J, Anker SD, Haehling S von. Growth hormone secretagogues: history, mechanism of action, and clinical development. JCSM Rapid Commun. 2020;3:25–37.
Janvier S, Cheyns K, Canfyn M, Goscinny S, Spiegeleer BD, Vanhee C, et al. Impurity profiling of the most frequently encountered falsified polypeptide drugs on the Belgian market. Talanta. 2018;188:795-807.
Józwiak M, Bauer M, Kamysz W, Kleczkowska P. Multifunctionality and Possible Medical Application of the BPC 157 Peptide—Literature and Patent Review. Pharmaceuticals. 2025;18:185.
Karacabeyli D, Lacaille D. Glucagon-like peptide-1 receptor agonists in arthritis: current insights and future directions. Nat Rev Rheumatol. 2025;21:671–83.
Kingsberg SA, Clayton AH, Portman D, et al. Bremelanotide for the Treatment of Hypoactive Sexual Desire Disorder: Two Randomized Phase 3 Trials. Obstet Gynecol. 2019;134(5):899-908.
Kovalzon VM, Strekalova TV. Delta sleep-inducing peptide (DSIP): a still unresolved riddle. J Neurochem. 2006;97(2):303-309.
Kruger THC, Deiter F, Zhang Y, et al. Effects of Intranasal Oxytocin Administration on Sexual Functions in Healthy Women: A Laboratory Paradigm. J Clin Psychopharmacol. 2018;38(3):239-242.
Lee C, Zeng J, Drew BG, Sallam T, Martin-Montalvo A, Wan J, et al. The Mitochondrial-Derived Peptide MOTS-c Promotes Metabolic Homeostasis and Reduces Obesity and Insulin Resistance. Cell Metab. 2015;21:443–54.
Lee E, Padgett B. Intra-Articular Injection of BPC 157 for Multiple Types of Knee Pain. Altern Ther Heal Med. 2021;27:8–13.
Márquez-Cruz M, Kammar-García A, Huerta-Cruz JC, Carrasco-Portugal M del C, Barranco-Garduño LM, Rodríguez-Silverio J, et al. Three- and six-month efficacy and safety of phentermine in a Mexican obese population. Int J Clin Pharmacol Ther. 2021;59:539–48.
Mathioudakis AG, Chatzimavridou-Grigoriadou V, Evangelopoulou E, Mathioudakis GA. Vasoactive intestinal peptide inhaled agonists: potential role in respiratory therapeutics. Hippokratia. 2013;17(1):12-16.
McGuire FP, Martinez R, Lenz A, Skinner L, Cushman DM. Regeneration or Risk? A Narrative Review of BPC-157 for Musculoskeletal Healing. Curr Rev Musculoskelet Med. 2025;18:611-619.
Mead MP, Gumucio JP, Awan TM, Mendias CL, Sugg KB. Pathogenesis and management of tendinopathies in sports medicine. Transl Sports Med. 2018;1:5-13.
Mendias CL, Awan TM. Safety and efficacy of approved and unapproved peptide therapies for musculoskeletal injuries and athletic performance. Sports Med. 2026, accepted.
Mendias CL, Enselman ERS, Olszewski AM, Gumucio JP, Edon DL, Konnaris MA, et al. The Use of Recombinant Human Growth Hormone to Protect Against Muscle Weakness in Patients Undergoing Anterior Cruciate Ligament Reconstruction: A Pilot, Randomized Placebo-Controlled Trial. Am J Sports Med. 2020;48:1916–28.
Mills EG, Ertl N, Wall MB, et al. Effects of Kisspeptin on Sexual Brain Processing and Penile Tumescence in Men With Hypoactive Sexual Desire Disorder: A Randomized Clinical Trial. JAMA Netw Open. 2023;6(2):e2254313.
Otvos L, Wade JD. Big peptide drugs in a small molecule world. Front Chem. 2023;11:1302169.
Pickart L, Margolina A. Skin Regenerative and Anti-Cancer Actions of Copper Peptides. Cosmetics. 2018;5:29.
Prakash A, Goa KL. Sermorelin. BioDrugs. 1999;12:139–57.
Raun K, Hansen BS, Johansen NL, Thogersen H, Madsen K, Ankersen M, et al. Ipamorelin, the first selective growth hormone secretagogue. Eur J Endocrinol. 1998;139:552–61.
Ricke J-N, Seifert R. Disinformation on dietary supplements by German influencers on Instagram. Naunyn-Schmiedeberg’s Arch Pharmacol. 2025;398:5629–47.
Saueressig T, Owen PJ, Pedder H, Tagliaferri S, Kaczorowski S, Altrichter A, et al. The importance of context (placebo effects) in conservative interventions for musculoskeletal pain: A systematic review and meta‐analysis of randomized controlled trials. Eur J Pain. 2024;28:675–704.
Sharma A, Kumar A, Torre BG de la, Albericio F. Liquid-Phase Peptide Synthesis (LPPS): A Third Wave for the Preparation of Peptides. Chem Rev. 2022;122:13516–46.
Shen Y, Liu M, Botchway BOA, Zhang Y, Liu X. Molecular mechanisms of cuproptosis in osteoarthritis: Pathways, crosstalk, and therapeutic opportunities. Exp Cell Res. 2025;453:114800.
Sosne G, Qiu P, Goldstein AL, Wheater M. Biological activities of thymosin ß4 defined by active sites in short peptide sequences. FASEB J. 2010;24:2144–51.
Stier. Safety and Tolerability of the Hexadecapeptide AOD9604 in Humans. J Endocrinol Metab. 2013.
Teichman SL, Neale A, Lawrence B, Gagnon C, Castaigne J-P, Frohman LA. Prolonged Stimulation of Growth Hormone (GH) and Insulin-Like Growth Factor I Secretion by CJC-1295, a Long-Acting Analog of GH-Releasing Hormone, in Healthy Adults. J Clin Endocrinol Metab. 2006;91:799–805.
Thurston L, Hunjan T, Ertl N, et al. Effects of Kisspeptin Administration in Women With Hypoactive Sexual Desire Disorder: A Randomized Clinical Trial. JAMA Netw Open. 2022;5(10):e2236131.
Tung C, Varzideh F, Farroni E, Mone P, Kansakar U, Jankauskas SS, et al. Elamipretide: A Review of Its Structure, Mechanism of Action, and Therapeutic Potential. Int J Mol Sci. 2025;26:944.
Turnock DL, Gibbs DN. Click, click, buy: The market for novel synthetic peptide hormones on mainstream e-commerce platforms in the UK. Perform Enhanc Heal. 2023;11:100251.
Vasireddi N, Hahamyan H, Salata MJ, Karns M, Calcei JG, Voos JE, et al. Emerging Use of BPC-157 in Orthopaedic Sports Medicine: A Systematic Review. HSS J. 2025;21:485–95.
Viennois E, Ingersoll SA, Ayyadurai S, et al. Critical role of PepT1 in promoting colitis-associated cancer and therapeutic benefits of the anti-inflammatory PepT1-mediated tripeptide KPV in a murine model. Cell Mol Gastroenterol Hepatol. 2016;2(3):340-357.
Wang L, Wang N, Zhang W, Cheng X, Yan Z, Shao G, et al. Therapeutic peptides: current applications and future directions. Signal Transduct Target Ther. 2022;7:48.
Wessells H, Fuciarelli K, Hansen J, Hadley ME, Hruby VJ, Dorr R. Synthetic melanotropic peptide initiates erections in men with psychogenic erectile dysfunction: double-blind, placebo controlled crossover study. J Urol. 1998;160(2):389-393.
Wessells H, Levine N, Hadley ME, Dorr R, Hruby V, Dorr R. Effect of an alpha-melanocyte stimulating hormone analog on penile erection and sexual desire in men with organic erectile dysfunction. Urology. 2000;56(4):641-646.
Zheng Y, Wei Z, Wang T. MOTS-c: A promising mitochondrial-derived peptide for therapeutic exploitation. Front Endocrinol. 2023;14:1120533.