Understanding Post-Finasteride Syndrome: Causes, Symptoms, and Treatment Approaches
What Is Post-Finasteride Syndrome?
Post-finasteride syndrome, often abbreviated PFS, is a term used to describe persistent sexual, neurological, psychological, physical, and hormonal symptoms that continue after stopping finasteride. Finasteride is a 5-alpha-reductase inhibitor commonly prescribed for androgenic alopecia, or male pattern hair loss, and benign prostatic hyperplasia, or prostate enlargement.
Finasteride can be effective for reducing hair loss and improving urinary symptoms in selected patients. It works by lowering dihydrotestosterone, or DHT, a potent androgen formed from testosterone. For most patients who use finasteride, side effects are either absent or improve after stopping the medication. However, a subset of patients report persistent symptoms that last for months or years after discontinuation.
PFS remains medically complex and incompletely understood. There is no universally accepted diagnostic test, no single biomarker, and no standard treatment protocol that works for every patient. This does not mean symptoms should be dismissed. It means patients need careful evaluation, a thoughtful differential diagnosis, and an individualized treatment plan.
How Finasteride Works
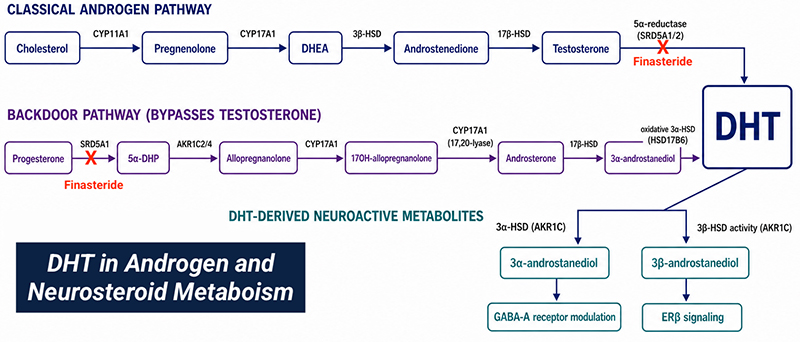
Finasteride blocks 5-alpha-reductase, the enzyme that converts testosterone into DHT. DHT is important in hair follicles, prostate tissue, skin, genital tissue, and other androgen-sensitive tissues. In the scalp, reducing DHT can slow miniaturization of hair follicles in androgenic alopecia. In the prostate, reducing DHT can shrink prostate tissue and improve urinary symptoms in some men.
The 5-alpha-reductase system is not limited to hair and prostate tissue. It also participates in the metabolism of several steroid hormones, including progesterone and other neurosteroid precursors. These pathways help produce neuroactive steroids such as allopregnanolone, which can influence GABA signaling, mood, sleep, stress response, cognition, and sexual function.
This is one reason PFS is thought to be more than a simple testosterone or DHT problem. In some patients, persistent symptoms may involve endocrine signaling, neurosteroid pathways, androgen receptor sensitivity, sexual tissue function, pelvic floor function, autonomic regulation, and psychological adaptation to chronic symptoms.
Why PFS is Difficult to Diagnose
PFS is challenging because symptoms overlap with many other conditions. Low libido, erectile dysfunction, brain fog, fatigue, anxiety, depression, insomnia, poor exercise recovery, and body composition changes can also occur with low testosterone, sleep apnea, thyroid dysfunction, depression, chronic stress, overtraining, medication effects, pelvic floor dysfunction, diabetes, obesity, cardiovascular disease, or other medical conditions.
There is also no blood test that confirms PFS. Testosterone, DHT, LH, FSH, estradiol, prolactin, thyroid markers, metabolic labs, and inflammatory markers may provide useful information, but they do not prove or disprove the diagnosis by themselves.
For many patients, the diagnosis is clinical. It depends on the timing of symptoms, the relationship to finasteride exposure, persistence after discontinuation, symptom pattern, and exclusion of other treatable contributors.
A careful clinician should avoid two extremes. The first is dismissing symptoms because PFS is not fully understood. The second is assuming every symptom is caused by finasteride without evaluating other medical, hormonal, metabolic, pelvic, sleep, and psychological contributors. The best approach is to take the symptoms seriously and investigate systematically.
Common Symptoms
Symptoms reported after finasteride exposure often occur in clusters. They may be sexual, neurologic, psychological, physical, or hormonal.
Sexual symptoms may include:
- Low libido
- Erectile dysfunction
- Reduced morning erections
- Reduced genital sensation or penile numbness
- Difficulty with arousal
- Orgasmic changes
- Reduced pleasure or sexual anhedonia
- Reduced semen volume
- Ejaculatory changes
- Penile tissue changes or perceived genital changes
- Infertility concerns in selected patients
Neurological and cognitive symptoms may include:
- Brain fog
- Poor concentration
- Memory difficulty
- Reduced motivation
- Emotional blunting
- Sleep disruption
- Head pressure or altered sensory symptoms
- Reduced stress tolerance
Psychological symptoms may include:
- Anxiety
- Depression
- Panic symptoms
- Anhedonia
- Irritability
- Low confidence
- Distress related to sexual changes
- Relationship stress
- Suicidal thoughts in severe cases
Physical symptoms may include:
- Fatigue
- Reduced exercise tolerance
- Muscle loss or difficulty building muscle
- Increased fat mass
- Dry skin
- Changes in body hair
- Gynecomastia or breast tenderness
- Testicular discomfort
- Pelvic pain or pelvic floor tension
Hormonal or reproductive findings may include:
- Low-normal testosterone
- Low DHT in some patients
- Altered estradiol balance
- Changes in LH or FSH
- Abnormal semen parameters in selected patients
- Low libido or erectile symptoms despite apparently “normal” labs
Symptoms can fluctuate. Some patients report waves, crashes, partial improvements, setbacks after stress or illness, or changes related to sleep, exercise, sexual activity, medications, or supplements.
Role of DHT in Systemic Physiology
DHT is often thought of only as a hair-loss hormone, but it has broader roles in male physiology. DHT is a potent androgen that binds strongly to androgen receptors in certain tissues. It contributes to development and maintenance of male genital tissue, prostate biology, skin and hair follicle signaling, sexual function, and aspects of androgen-sensitive physiology.
Finasteride lowers DHT by blocking conversion of testosterone to DHT. In many patients, this is tolerated well. In others, reduced DHT signaling may contribute to sexual side effects such as lower libido, erectile changes, reduced ejaculatory volume, or altered genital sensation.
However, PFS is unlikely to be explained only by low DHT. Some patients have persistent symptoms even when serum hormone levels appear normal. This suggests that tissue-level androgen signaling, receptor sensitivity, neurosteroid changes, nervous system regulation, pelvic floor function, and psychological distress may all matter.
Neurosteroids and GABA Signaling
One of the most important proposed mechanisms in PFS involves neurosteroids. Neurosteroids are steroid-derived molecules that influence brain and nervous system function. Some neurosteroids, including allopregnanolone, modulate GABA-A receptor activity. GABA is one of the brain’s main inhibitory neurotransmitter systems and is involved in calmness, sleep, anxiety regulation, stress response, and mood stability.
Because 5-alpha-reductase participates in neurosteroid metabolism, finasteride may affect more than DHT. It can alter pathways involved in progesterone-derived neurosteroids and other steroid metabolites. In susceptible individuals, this may contribute to anxiety, insomnia, emotional blunting, depression, cognitive symptoms, and altered stress response.
This mechanism remains an area of active research. It does not explain every case, and it does not mean every patient should take neurosteroid supplements or GABA-active medications. It does support the idea that PFS symptoms may involve the brain and nervous system as well as the endocrine system.
Androgen Receptor and Tissue Sensitivity
Another proposed mechanism is altered androgen receptor signaling. The androgen receptor is the cellular receptor that responds to testosterone and DHT. If receptor sensitivity, density, gene expression, or downstream signaling changes, a patient may experience symptoms even when blood hormone levels look normal.
This may help explain why some patients report persistent sexual or physical symptoms despite testosterone values that are technically within range. A lab value does not always capture tissue-level hormone response.
At this time, androgen receptor changes in PFS are not easy to measure in routine clinical practice. Treatment should therefore focus on identifying modifiable contributors: testosterone status, DHT status when appropriate, estradiol balance, metabolic health, sleep, pelvic floor function, erectile tissue health, cardiovascular risk, and mental health.
Autonomic Nervous System Dysregulation
Some patients with PFS describe symptoms that suggest autonomic nervous system involvement: anxiety surges, insomnia, palpitations, sweating changes, sexual dysfunction, reduced arousal response, digestive changes, pelvic tension, or feeling stuck in a high-alert state.
The autonomic nervous system regulates erection, ejaculation, heart rate, digestion, sweating, blood pressure, and stress response. Sexual function requires coordination between psychological arousal, parasympathetic activity, sympathetic activity, vascular function, sensory input, pelvic floor control, and hormone signaling.
When the nervous system is dysregulated, patients may experience sexual dysfunction even when hormone levels are not dramatically abnormal. This is why rehabilitation, breathwork, sleep optimization, pelvic floor treatment, and stress regulation may be useful parts of care.
Pelvic Floor and Sexual Function
PFS is often discussed as a hormone or neurosteroid condition, but pelvic floor function should not be overlooked. Erectile function, ejaculation, genital sensation, pelvic comfort, and sexual confidence are all influenced by the pelvic floor, pudendal nerve, hips, low back, breathing mechanics, and autonomic nervous system.
Men with persistent sexual symptoms may develop guarding, avoidance, performance anxiety, pelvic floor overactivity, or reduced confidence. Others may have pelvic pain, urinary symptoms, premature ejaculation, delayed ejaculation, or genital numbness that overlaps with pelvic floor dysfunction.
Pelvic floor rehabilitation is not just Kegels. In many men, especially those with pain, tightness, urinary urgency, or genital sensitivity changes, the first step may be relaxation, downtraining, breathing, mobility, manual therapy, neuromuscular retraining, and gradual sexual function rehabilitation.
Erectile Dysfunction After Finasteride
Erectile dysfunction in suspected PFS can have multiple contributors. These may include altered androgen signaling, reduced libido, impaired arousal, vascular risk factors, pelvic floor dysfunction, anxiety, depression, poor sleep, metabolic disease, or loss of confidence after repeated difficult sexual experiences.
Evaluation should include erectile quality, morning erections, libido, orgasm quality, genital sensation, relationship context, medication history, cardiometabolic risk, and hormone labs.
Treatment may include PDE5 inhibitors such as tadalafil or sildenafil when appropriate, testosterone optimization when indicated, pelvic floor rehabilitation, shockwave therapy in selected ED patients, sexual counseling, sleep optimization, and metabolic risk reduction.
The goal is to restore sexual function as a system, not to assume one medication or one hormone will solve every case.
Mood, Anxiety, and Mental Health
PFS can be emotionally distressing. Sexual dysfunction, genital sensation changes, brain fog, fatigue, insomnia, and uncertainty about recovery can all affect mood and identity. Some patients also report anxiety, depression, emotional blunting, or anhedonia that they believe began during or after finasteride exposure.
Mental health symptoms should be treated seriously. This does not mean symptoms are “just psychological.” It means the brain, endocrine system, sexual function, sleep, and stress physiology are interconnected.
Patients with severe depression, suicidal thoughts, panic symptoms, or inability to function should receive urgent mental health support. Treatment may include therapy, psychiatry, medication review, sleep treatment, nervous system regulation, exercise rehabilitation, social support, and careful coordination with medical care.
Fertility and Semen Parameters
Finasteride can affect semen volume and sperm parameters in some men, although effects often improve after discontinuation. In patients with persistent fertility concerns, semen analysis is the most useful starting point.
A fertility-focused evaluation may include semen analysis, testosterone, LH, FSH, estradiol, prolactin, thyroid testing, medication review, varicocele assessment, sleep and metabolic evaluation, and referral to reproductive urology when appropriate.
Men actively trying to conceive should avoid experimenting with hormonal medications, testosterone, SERMs, hCG, or supplements without medical supervision. Some treatments can improve symptoms but worsen fertility, while others may support fertility depending on the clinical context.
Initial Evaluation
A comprehensive evaluation for suspected PFS should look beyond one hormone panel. Depending on symptoms, testing may include:
- Total testosterone
- Free testosterone
- SHBG
- DHT when clinically useful
- LH and FSH
- Estradiol
- Prolactin
- DHEA-S
- Pregnenolone when appropriate
- Thyroid testing
- CBC and CMP
- Lipid panel
- Hemoglobin A1c and fasting glucose
- Vitamin D
- B12 and folate when fatigue or neurologic symptoms are present
- Ferritin and iron studies when fatigue is present
- hs-CRP or other inflammation markers when appropriate
- Semen analysis when fertility is a concern
- Sleep apnea screening
- Mental health screening
- Pelvic floor and sexual function assessment for patients with erectile or other sexual dysfunction
Not every patient needs every test. The workup should be matched to symptoms, duration, age, medications, fertility goals, and risk factors.
Hormonal Treatment Considerations
There is no universally accepted hormonal treatment for PFS. Some patients may have clear hypogonadism and benefit from testosterone therapy. Others may have normal testosterone but altered libido, erectile function, or DHT-related symptoms. Some may have fertility goals that make testosterone therapy inappropriate.
Possible hormonal strategies discussed in clinical practice may include:
- Testosterone therapy in documented hypogonadism
- hCG when fertility preservation or testicular signaling is relevant
- SERMs such as clomiphene or enclomiphene in selected men
- Estradiol management when clearly abnormal
- DHEA or pregnenolone support in selected cases
- Avoidance of unnecessary aromatase inhibitor use
- Careful monitoring of symptoms and labs
These approaches should not be used casually. Hormonal manipulation can create new problems if the diagnosis is wrong, dosing is excessive, estradiol is over-suppressed, fertility goals are ignored, or psychiatric symptoms are unstable.
Neurosteroid and Nervous System Support
Because neurosteroid changes are one proposed mechanism, some patients ask about pregnenolone, progesterone pathways, allopregnanolone analogs, GABA-active medications, or other neuroactive treatments.
This area is still investigational. Some patients may respond to carefully selected therapies, but others may worsen with aggressive supplement or medication trials. GABA-active medications such as benzodiazepines carry dependency and tolerance risks and should be used only when clinically appropriate and carefully monitored.
A safer foundation often includes sleep treatment, breathwork, nervous system regulation, gradual exercise, nutrition support, treatment of anxiety or depression, and avoidance of overstimulating supplement stacks.
Mitochondrial and Metabolic Support
Fatigue, brain fog, and poor exercise tolerance are common complaints in suspected PFS. These symptoms may involve sleep disruption, depression, deconditioning, low testosterone, altered neurosteroids, inflammation, metabolic dysfunction, or nutritional deficiencies.
Some patients may benefit from mitochondrial and metabolic support, but this should be framed realistically. Supplements such as creatine, CoQ10, L-carnitine, vitamin D, magnesium, omega-3 fatty acids, and B vitamins may be useful when matched to symptoms, labs, and nutrition status. They are not proven cures for PFS.
The most evidence-based metabolic foundation includes resistance training, aerobic conditioning, adequate protein, sleep, body composition improvement, glucose control, and treatment of sleep apnea or metabolic disease when present.
Exercise and Body Composition
Some men with PFS report muscle loss, fat gain, reduced exercise tolerance, or poor recovery. A structured exercise plan can help rebuild confidence, improve insulin sensitivity, support testosterone physiology, improve mood, and restore physical capacity.
The plan should be gradual. Patients who are highly symptomatic may not tolerate aggressive training at first. Overtraining can worsen fatigue, insomnia, anxiety, and sexual symptoms.
Some common components of an exercise plan may include:
- Progressive resistance training
- Zone 2 aerobic conditioning
- Mobility work
- Pelvic floor coordination when relevant
- Recovery days
- Sleep tracking
- Protein and calorie adequacy
- Body composition monitoring
The goal is not to punish the body into recovery. The goal is to restore capacity through repeated, tolerable, measurable progress.
Sleep Optimization
Sleep is central to sexual function, testosterone production, mood regulation, cognitive function, metabolic health, and nervous system recovery. Insomnia is common in many chronic symptom syndromes and may be especially distressing in suspected PFS.
Sleep evaluation should include bedtime timing, wake time, alcohol, caffeine, screen exposure, anxiety, snoring, oxygen drops, sleep apnea risk, restless legs, medications, and supplements.
Treating sleep apnea, improving circadian rhythm, reducing late stimulants, using breathwork, and addressing anxiety can sometimes improve multiple symptoms at once.
Nutrition and Gut Health
Nutrition can influence hormone metabolism, inflammation, gut function, blood sugar, and energy. Patients with persistent symptoms often try restrictive diets or large supplement stacks. Sometimes this helps. Sometimes it worsens stress, under-fueling, and anxiety.
Typical components of a nutrition and gut health program for patients with PFS can include:
- Adequate protein
- Fiber-rich carbohydrates
- Colorful vegetables and fruit
- Healthy fats
- Omega-3-rich foods
- Adequate calories
- Hydration
- Limiting alcohol
- Minimizing ultra-processed foods
Patients with GI symptoms, reflux, constipation, diarrhea, or bloating may need additional evaluation rather than assuming everything is hormone-related.
What Patients Should Avoid
Patients should avoid high-risk self-experimentation. When symptoms are severe, it is understandable to search online for protocols, but aggressive trial-and-error can worsen symptoms and make it harder to identify what helps. Things most patients should avoid include:
- Restarting or stopping hormonal medications without medical guidance
- Unsupervised testosterone, hCG, SERMs, or aromatase inhibitors outside of medical guidance
- High-dose neurosteroid or GABA-active supplements without monitoring or medical guidance
- Excessive supplement stacking
- Internet protocols that promise a cure
- Ignoring depression or suicidal thoughts
- Overtraining to force recovery
- Dismissing pelvic floor symptoms
- Assuming all symptoms are permanent
The goal is careful, stepwise treatment with tracking and reassessment.
A Practical Treatment Framework
Because PFS is complex, treatment should be organized rather than random.
- First, document the timeline. When was finasteride started? When did symptoms begin? Did they occur during treatment or after stopping? Which symptoms persisted?
- Second, identify the dominant symptom cluster. Is the primary problem sexual dysfunction, low libido, erectile dysfunction, insomnia, anxiety, fatigue, cognitive symptoms, body composition change, pelvic pain, or fertility?
- Third, evaluate other contributors. Sleep apnea, low testosterone, thyroid disease, diabetes risk, depression, medication effects, pelvic floor dysfunction, and nutritional deficiencies should be considered.
- Fourth, treat the most modifiable problems first. These may include sleep, erectile function, pelvic floor dysfunction, hypogonadism, metabolic health, anxiety, depression, nutrition, and deconditioning.
- Fifth, use advanced or experimental strategies cautiously. Neurosteroid or biologic approaches should be considered only after risk, uncertainty, and goals are discussed.
- Sixth, reassess. Symptoms, labs, sexual function, sleep, mood, training tolerance, and quality of life should be tracked over time.
When To Seek Urgent Help
Urgent help is needed if a patient has suicidal thoughts, plans for self-harm, severe depression, panic symptoms that feel unsafe, inability to sleep for multiple nights, chest pain, fainting, severe neurologic symptoms, or rapidly worsening mental health.
Persistent sexual symptoms are important, but safety comes first. Patients should not try to manage severe psychiatric symptoms alone.
A Better Way to Approach PFS
Post-finasteride syndrome is difficult because it sits at the intersection of hormones, neurosteroids, sexual function, mood, sleep, metabolism, pelvic health, and nervous system regulation. Patients often feel dismissed, confused, or left to manage symptoms alone.
The best approach is comprehensive and careful. There may not be one universal cure, but there are often treatable contributors that can be identified and addressed.
At the Performance Medicine Institute, we take a comprehensive approach to suspected post-finasteride syndrome by combining endocrine evaluation, sexual health assessment, pelvic floor rehabilitation, metabolic testing, sleep screening, body composition evaluation, mental health support, erectile function treatment, and individualized recovery planning. Contact us to schedule an evaluation.
References
- Giatti S, Diviccaro S, Panzica G, Melcangi RC. Post-finasteride syndrome and post-SSRI sexual dysfunction: two clinical conditions apparently distant, but very close. Front Neuroendocrinol. 2018;51:10-24.
- Irwig MS. Persistent sexual side effects of finasteride: could they be permanent? J Sex Med. 2012;9(11):2927-2932.
- Kiguradze T, Temps WH, Yarnold PR, et al. Persistent erectile dysfunction in men exposed to the 5-alpha reductase inhibitors finasteride or dutasteride. PeerJ. 2017;5:e3020.
- Melcangi RC, Santi D, Spezzano R, et al. Neuroactive steroid levels and psychiatric and andrological features in post-finasteride patients. J Steroid Biochem Mol Biol. 2017;171:229-235.
- Melcangi RC, Caruso D, Abbiati F, et al. Post-finasteride syndrome: an emerging clinical problem. Neurobiol Stress. 2020;12:100209.
- Motta G, Negri-Cesi P, Poletti A, Melcangi RC. Steroid metabolism in the brain: role of 5-alpha-reductase and 3-alpha-hydroxysteroid oxidoreductase in androgen and progestin action. J Steroid Biochem Mol Biol. 1997;61(3-6):217-226.
- Nguyen DD, Marchese M, Cone EB, et al. Investigation of suicidality and psychological adverse events in patients treated with finasteride. JAMA Dermatol. 2021;157(1):35-42.
- Pereira AFJR, Coelho TOA. Post-finasteride syndrome. An Bras Dermatol. 2020;95(3):271-277.
- Sohn M, Lee HY, Lim JS, et al. Sexual, physical, and overall adverse effects in patients treated with 5-alpha-reductase inhibitors: a systematic review and meta-analysis. World J Mens Health. 2022;40(4):665-675.
- Traish AM. The post-finasteride syndrome: clinical manifestation of drug-induced epigenetics due to endocrine disruption. Curr Sex Health Rep. 2018;10:88-103.
- Traish AM. The impact of 5-alpha-reductase inhibitors on male sexual function and psychological well-being. Asian J Androl. 2018;20(3):221-228.